| Table 1. Selected Evidence Informing NCCN Adverse Risk Factors in Merkel Cell Carcinoma | ||
| Studies informing adverse clinicopathologic features commonly used in postoperative radiation therapy decision-making. | ||
| Key Study | Design / N | Principal Finding Relevant to Risk Factor |
|---|---|---|
| Lymphovascular Invasion | ||
| Fields et al. (MSKCC) (2011) | Retrospective, n = 153 | Patients with LVI were more likely to have a positive SLNB. No patient without LVI experienced recurrence or MCC-specific death in this cohort. |
| Conic et al. (NCDB) (2019) | Population-based, n = 3,048 | LVI was associated with greater odds of SLN positivity (OR 3.45, p < 0.001) and was the strongest predictor evaluated. |
| Harounian et al. (2021) | Retrospective, n = 122 | Compared with patients without LVI, those with LVI had worse RFS (HR 2.3, p = 0.04), worse DSS (HR 5.2, p = 0.007), and more frequent SLN positivity (62.0% vs. 25.5%, p = 0.003). |
| Bartlett et al. (MSKCC) (2026) | Retrospective, n = 342 | Tumors with LVI and tumors >2 cm were more likely to have a positive SLN on multivariable analysis. |
| Immunosuppression | ||
| Liang et al. (U. Wisconsin) (2015) | Retrospective, n = 87 | Immunosuppressed patients had worse survival than immunocompetent patients (HR 2.01, 95% CI 1.1–3.7). |
| Yusuf et al. (NCDB) (2021) | Population-based, n = 3,882 | Immunosuppressed patients had worse 3-year OS than immunocompetent patients (44.6% vs. 68.7%, p < 0.0001; adjusted mortality HR 2.36, 95% CI 2.03–2.75). Among immunosuppressed patients, solid-organ transplant recipients had the lowest 3-year OS (32.7%). |
| McEvoy et al. (Seattle) (2022) | Prospective cohort, n = 618 | Immunosuppressed patients had a higher risk of recurrence than immunocompetent patients (HR 2.4, 95% CI 1.7–3.3, p < 0.001). |
| Primary Tumor >1 cm | ||
| Stokes et al. (VA) (2009) | VA database, n = 346 | Regional lymph-node metastasis was less frequent for tumors ≤1 cm than for tumors >1 cm (4% vs. 24%, p < 0.0001). |
| Smith et al. (Moffitt) (2015) | Retrospective, n = 375 | Increasing tumor diameter was associated with greater SLN positivity (p = 0.007), worse OS (p = 0.003), and worse DSS (p = 0.008). |
| Bartlett et al. (MSKCC) (2026) | Retrospective, n = 342 | Even among patients with tumors ≤1 cm and no LVI, 17% had a positive SLN, indicating that small size alone did not exclude occult nodal disease. |
| Close/Positive Margins | ||
| Andruska et al. (Wash U) (2021) | Retrospective, n = 79 stage I–II | Patients with close or positive margins ≤3 mm had worse distant RFS (HR 6.83, 95% CI 1.80–25.9). Each additional 1 cm of WLE margin was associated with improved regional RFS, distant RFS, and DSS. |
| Tarabadkar et al. (Seattle) (2021) | Retrospective, n = 188 | Among patients receiving adjuvant RT, local recurrence was approximately 1% regardless of margin width. Without RT, local recurrence was 20% after margins ≤1 cm versus 0% after margins >1 cm (p = 0.049). |
| Lodde et al. (DeCOG) (2025) | Multicenter, n = 1,049 | Margins of 1–2 cm were associated with the most favorable outcomes; margins >2 cm provided no additional observed benefit. |
| Kavanagh et al. (MSKCC) (2026) | Retrospective, n = 447 | Among patients treated with negative-margin surgery alone, the estimated 1-year local recurrence rate was 1.8%. |
| Positive SLNB | ||
| Servy et al. (2016) | Retrospective, n = 87 successful SLNB | Patients with a negative SLNB had longer DFS and OS than patients with a positive SLNB on multivariable analysis. |
| Harounian et al. (2021) | Retrospective, n = 122 | Patients with a positive SLN had worse RFS than patients with a negative SLN (HR 3.6, p = 0.007). |
| Ahn et al. (Westmead) (2026) | Retrospective, n = 75 | SLNB was positive in 37% of patients. Among patients with nodal disease, the overall false-negative rate was approximately 20%. |
| Bartlett et al. (MSKCC) (2026) | Retrospective, n = 342 | Patients with a positive SLN had a higher 5-year recurrence rate than patients with a negative SLN (39% vs. 12%, p < 0.001); SLN status was the only independent recurrence predictor identified. |
| Head/Neck Primary Site | ||
| Cullison et al. (SEER) (2021) | Population-based, n = 9,407 | Among patients with localized MCC, scalp or neck primary site was associated with the highest 5-year cumulative incidence of MCC-specific mortality, approximately 26%. |
| McEvoy et al. (Seattle) (2022) | Prospective cohort, n = 618 | Anatomic site was not significantly associated with recurrence in this cohort (p = 0.44), in which adjuvant RT was used frequently. |
| Nayak et al. (Pan-Canadian) (2023) | Multicenter, n = 400 head/neck MCC | In this head and neck MCC cohort, 5-year OS was 42%, and approximately one-half of patients experienced recurrence within 5 years. |
| Brenner et al. (Israel) (2025) | Multicenter, n = 191 | Patients with head and neck primaries had worse 5-year OS than patients with primaries at other anatomic sites (51.6% vs. 65.2%, p = 0.025; adjusted mortality HR 1.77, 95% CI 1.10–2.84, p = 0.018). |
| Wang et al. (2026) | Single-center cohort, n = 86 | For head and neck MCC, SLNB sensitivity was 52.6%. Among patients with nodal disease who underwent SLNB, the false-negative rate was 26.7%; SLNB mapping or identification failed in 29.0%. |
| The table is organized by the adverse clinicopathologic feature each study helps inform. Selected studies evaluated recurrence, sentinel lymph-node positivity, disease-specific survival, overall survival, surgical margins, or anatomic site; not all evaluated primary-site local recurrence as a discrete endpoint. | ||
| Abbreviations: CI, confidence interval; DeCOG, Dermatologic Cooperative Oncology Group; DFS, disease-free survival; DSS, disease-specific survival; HR, hazard ratio; LN, lymph node; LR, local recurrence; LVI, lymphovascular invasion; MCC, Merkel cell carcinoma; MSKCC, Memorial Sloan Kettering Cancer Center; NCDB, National Cancer Database; OR, odds ratio; OS, overall survival; RFS, recurrence-free survival; RT, radiation therapy; SLN, sentinel lymph node; SLNB, sentinel lymph node biopsy; VA, Veterans Affairs; WLE, wide local excision. | ||
Perspectives on the Science
Local Recurrence After Excision of Merkel Cell Carcinoma: What Do We Actually Know, and What Should We Do Next?
2026
Merkel Cell Carcinoma
Radiation Therapy
Local Recurrence
This Perspectives on the Science article summarizes a multidisciplinary Society of Cutaneous Oncology Journal Club discussion of Kavanagh et al., Local Recurrence Following Complete Surgical Excision of Primary Merkel Cell Carcinoma. The discussion examines uncertainty in local recurrence risk after margin-negative excision, variation in postoperative radiation therapy practice, and future evidence-generation approaches that integrate curated multi-institutional data, causal inference, and probabilistic modeling to support decision-making under uncertainty.
Kevin Scott Emerick, MD 
Howard Lane Kaufman, MD
Aubriana M. McEvoy, MD, MS
Lisa Zaba, MD, PhD
Ajay Sharma, MD
Adewunmi Adelaja, MD, PhD
Ann W. Silk, MD
Nikhil I. Khushalani, MD
Isaac Brownell, MD, PhD
Daniel G. Coit, MD
Paul Nghiem, MD, PhD
Vernon K Sondak, MD
Keywords
Merkel Cell Carcinoma, Local Recurrence, Adjuvant Radiation, Postoperative Radiation, Causal Inference
Featured Article
| Kavanagh, F. G. et al. Local Recurrence Following Complete Surgical Excision of Primary Merkel Cell Carcinoma. Annals of Surgical Oncology (2026).1 |
Introduction
The natural history of local recurrence after excision of localized Merkel cell carcinoma (MCC) remains incompletely defined. This uncertainty is not merely descriptive: it directly informs one of the most debated decisions in localized MCC management, namely whether adjuvant radiation therapy (RT) should be recommended after complete excision. Although postoperative RT is frequently considered for patients with adverse clinicopathologic features, substantial uncertainty persists regarding the baseline risk of local recurrence, the clinicopathologic factors that meaningfully modify that risk, the patients most likely to derive clinically meaningful benefit from treatment, and the outcomes of patients who develop local recurrence and undergo salvage therapy2–4. More fundamentally, this debate raises a broader scientific question: how should clinicians make evidence-based decisions when definitive evidence is unlikely to emerge in the foreseeable future?
Reported rates of local recurrence following excision of MCC vary substantially across the literature. Historical studies reinforced the perception that MCC carries a high risk of local recurrence at the primary site; in their 1991 review of 234 patients, Shaw and Rumball reported local recurrence after excision alone in 39% of patients5. By contrast, several more contemporary institutional cohorts have reported substantially lower local recurrence rates, often in the range of approximately 1–8%1,6–8. However, these estimates are not directly interchangeable. Published series differ with respect to patient selection, margin status, pathologic nodal evaluation, use or omission of adjuvant RT, definitions of local versus satellite, in-transit, or regional recurrence, and duration of follow-up. Consequently, clinicians are often asked to make treatment recommendations using recurrence estimates that differ by more than an order of magnitude, while recognizing that those estimates arise from different clinical eras, staging practices, treatment strategies, and endpoint definitions. The challenge, therefore, is not simply to identify a single “correct” recurrence rate, but to determine how best to reason and make decisions in the face of persistent uncertainty.
Against this background, Kavanagh and colleagues recently reported a large single-institution experience focused specifically on local recurrence following complete surgical excision of primary MCC1. The study is best understood as a natural-history analysis rather than a comparative trial of postoperative RT. Its clinical relevance, however, is direct: because primary-site RT is intended to prevent local recurrence, a focused estimate of that event inevitably informs radiation decision-making.
The clinical implications of this uncertainty are considerable. Current NCCN guidelines recommend consideration of postoperative RT for patients with adverse risk factors including lymphovascular invasion (LVI), immunosuppression, primary tumor size greater than 1 cm, close or positive margins, positive sentinel lymph node biopsy (SLNB), and head and neck primary site2. Yet the evidentiary basis supporting these recommendations remains heterogeneous (Table 1). Many of the risk factors incorporated into modern treatment algorithms were identified through retrospective studies designed to evaluate recurrence broadly, nodal positivity, disease-specific survival, or overall survival, rather than local recurrence specifically1,9–26. As a result, relatively few studies have been designed or adequately powered to determine which clinicopathologic features independently predict local recurrence after complete excision.
NoteTable 1. Selected evidence informing NCCN adverse risk factors in Merkel cell carcinoma
Thus, while the NCCN-listed adverse features used to guide postoperative RT recommendations are clinically reasonable and widely used, the evidence linking them specifically to local recurrence remains largely indirect. The challenge, therefore, is not simply that more evidence is needed. Rather, clinicians must make consequential treatment decisions using evidence that is incomplete, variably applicable, and unlikely to become definitive in the near future.
To explore how these evidence gaps are interpreted in practice, the Society of Cutaneous Oncology (SoCO) convened a multidisciplinary Journal Club bringing together dermatologists, medical oncologists, surgical oncologists, radiation oncologists, and trainees from across the MCC community. Here, we review the findings of Kavanagh et al., summarize survey results and expert discussion generated during that session, and consider how future evidence generation in MCC can support more rigorous decision-making under persistent uncertainty.
Evolution of the Evidence Base
Early Observations and the Emergence of Adjuvant Radiation
Much of the early literature describing recurrence patterns in MCC was generated across clinical eras that differed substantially in staging, pathologic evaluation, surgical management, use of adjuvant RT, and follow-up. Many historical series also predated routine SLNB-based nodal staging, which was incorporated into NCCN recommendations by 2006 and became increasingly integrated into practice after the first MCC-specific AJCC staging system was introduced in 20102,27,28. Recurrence estimates therefore varied widely across studies and often reflected mixed endpoints that combined local, regional, and distant failures. These reports, including the 1991 review by Shaw and Rumball, helped establish the perception that MCC was associated with a substantial risk of local recurrence after excision alone5.
In the absence of prospective randomized data, several institutional series and population-based analyses subsequently suggested that postoperative RT could improve local control and, in some reports, overall survival6,29–31. These studies contributed to the increasing adoption of adjuvant RT and established local control as a major therapeutic objective in localized MCC. However, interpretation of this literature remains constrained by retrospective design, inconsistent definitions of treatment and recurrence, variable follow-up, incomplete details regarding RT field, dose, and timing, and limited physician-curated review of recurrence events. As noted above, population-based registries provide complementary scale, but generally lack information on the date and site of first recurrence, salvage treatment, disease-specific survival, and competing causes of death. As a result, associations between adjuvant RT and improved overall survival in registry-based analyses should be interpreted cautiously and should not be assumed to establish a causal survival benefit.
Risk Stratification and Selective Radiation
As clinical practice became increasingly risk-adapted, the question evolved. Rather than asking only whether RT could improve local control, clinicians increasingly asked which patients were most likely to benefit after complete excision. During this period, adverse clinicopathologic features including lymphovascular invasion, immunosuppression, larger tumor size, positive SLNB, close or positive margins, and head and neck location emerged as important prognostic factors and were progressively incorporated into guideline recommendations3,7,13. Importantly, however, many of these features were identified as predictors of recurrence broadly, nodal involvement, systemic progression, disease-specific survival, or overall survival, rather than local recurrence specifically. Their use as indications for adjuvant RT therefore rests, in part, on the assumption that features associated with worse overall prognosis also identify patients at sufficiently increased risk of local recurrence to justify treatment.
At the same time, several institutional cohorts began reporting low rates of local recurrence among selected patients treated with complete excision and selective use or omission of adjuvant RT. Fields and colleagues reported a local recurrence rate of approximately 3% following complete resection, although 23% of patients received adjuvant local RT, making this a selective-therapy rather than surgery-alone recurrence estimate7. Frohm and colleagues observed only two true local or satellite recurrences among 104 patients managed without local RT, including one true local recurrence and one satellite recurrence, although the cohort was restricted to tumors smaller than 2 cm and reflected care at a high-volume center8. More recently, recurrence analyses from large prospective cohorts have reinforced that MCC recurrence risk varies substantially by stage and time from diagnosis, underscoring the need to interpret recurrence estimates in relation to patient and disease context13. Similarly, the observation arm of ADMEC-O provides a useful reminder that outcomes in completely resected MCC cohorts may differ from historical expectations, although its endpoint was disease-free survival rather than isolated local recurrence, and patients could receive other standard local therapies32. In this prospective randomized trial, local-regional relapse, not further subdivided, occurred in 10 of 61 patients on the observation arm after a minimum follow-up of 2 years for surviving patients, even though 74% of patients had received postoperative RT. Nevertheless, the investigators concluded that “the spontaneous course of MCC was better than historical data suggested”32.
These observations must be interpreted alongside a substantial body of retrospective evidence associating adjuvant RT with improved outcomes. In a systematic review and meta-analysis of 29 studies including 17,179 patients, Petrelli and colleagues found that adjuvant RT was associated with improved local disease-free survival, locoregional disease-free survival, and overall survival4. Similarly, Bhatia and colleagues, using the National Cancer Data Base, reported an association between adjuvant RT and improved overall survival in stage I and II MCC, although not in stage III disease3. However, registry-based overall survival analyses should be interpreted cautiously. Population-based registries generally lack information on the date and site of first recurrence, salvage treatment, and disease-specific survival, and overall survival is vulnerable to competing mortality and treatment-selection bias in early-stage MCC. Thus, reported associations between adjuvant RT and improved overall survival should not be assumed to establish a causal survival benefit.
More recent registry-based studies have also suggested that the timing of postoperative or adjuvant RT may be clinically important. In a prospective registry analysis of 124 patients with stage I/II MCC treated with postoperative RT, Alexander and colleagues found that initiation of RT more than 8 weeks after surgery was associated with increased locoregional recurrence and MCC-specific death33. Similarly, in the DeCOG multicenter registry of 1,049 patients, Lodde, Becker, and colleagues reported that delayed adjuvant RT was associated with poorer progression-free probability and disease-specific survival, while expansion of RT to the lymph node bed did not provide additional benefit21. These observational data do not eliminate concerns regarding treatment selection and confounding, but they suggest that timing, field selection, and patient risk may all matter.
Consequently, the available literature presents a persistent tension. Meta-analytic and registry-based studies report associations between adjuvant RT and improved outcomes, yet selected institutional cohorts report very low rates of local recurrence after complete excision, including among patients with adverse clinicopathologic features. Reconciling these observations requires greater clarity about the baseline risk of local recurrence, the clinical features that meaningfully modify that risk, the clinical consequences of local recurrence, and the absolute benefit that RT provides in different patient subgroups. This tension provides the immediate context for the Kavanagh study.
The Kavanagh Study
Study Overview
Kavanagh and colleagues addressed this question through a retrospective review of patients treated at Memorial Sloan Kettering Cancer Center over a four-decade period1. The investigators identified 447 patients with clinically localized MCC (no clinical evidence of nodal or distant metastasis at presentation) who underwent complete surgical excision with pathologically negative margins. Of these, 393 patients were managed with surgery alone, while 54 received adjuvant RT to the primary site. The authors focused specifically on local recurrence outcomes among patients managed without postoperative primary-site RT.
The study addressed a notable limitation of much of the existing literature. While numerous reports have evaluated recurrence broadly or examined the association between RT and clinical outcomes, relatively few have focused specifically on local recurrence after complete excision. By restricting the analysis to patients with pathologically negative margins and clearly defined local recurrence outcomes, Kavanagh and colleagues provided a more direct estimate of the event most relevant to decisions regarding postoperative primary-site RT.
Principal Findings
Among the 447 patients included in the study, only eight local recurrences were identified. All occurred among patients managed with surgery alone. Seven of the eight local recurrences occurred within the first year following treatment, yielding an estimated one-year local recurrence rate of 1.8% among the 393 patients managed without postoperative RT1.
Several observations deserve emphasis. First, local recurrence was uncommon. Second, local recurrences tended to occur early, consistent with broader MCC recurrence patterns in which recurrence risk is highest soon after diagnosis. Third, the clinical significance of local recurrence appeared to depend strongly on whether it occurred as an isolated event or in association with regional or distant disease. Among the six patients who developed isolated local recurrence, all achieved durable local control after additional local therapy. By contrast, the two patients who developed local recurrence with synchronous regional and distant metastatic disease died of disease, suggesting a biologically aggressive phenotype rather than a failure of local salvage alone. These findings raise important questions regarding the balance between recurrence prevention, salvageability, treatment burden, and RT-associated morbidity.
The study also highlights the challenges inherent in MCC outcomes research. Despite representing one of the largest institutional series focused specifically on local recurrence, only eight local recurrence events were observed. Given this low event rate, the study had limited ability to identify clinicopathologic predictors of local recurrence or to precisely estimate recurrence risk within individual subgroups.
Persistent Uncertainty in Current Practice
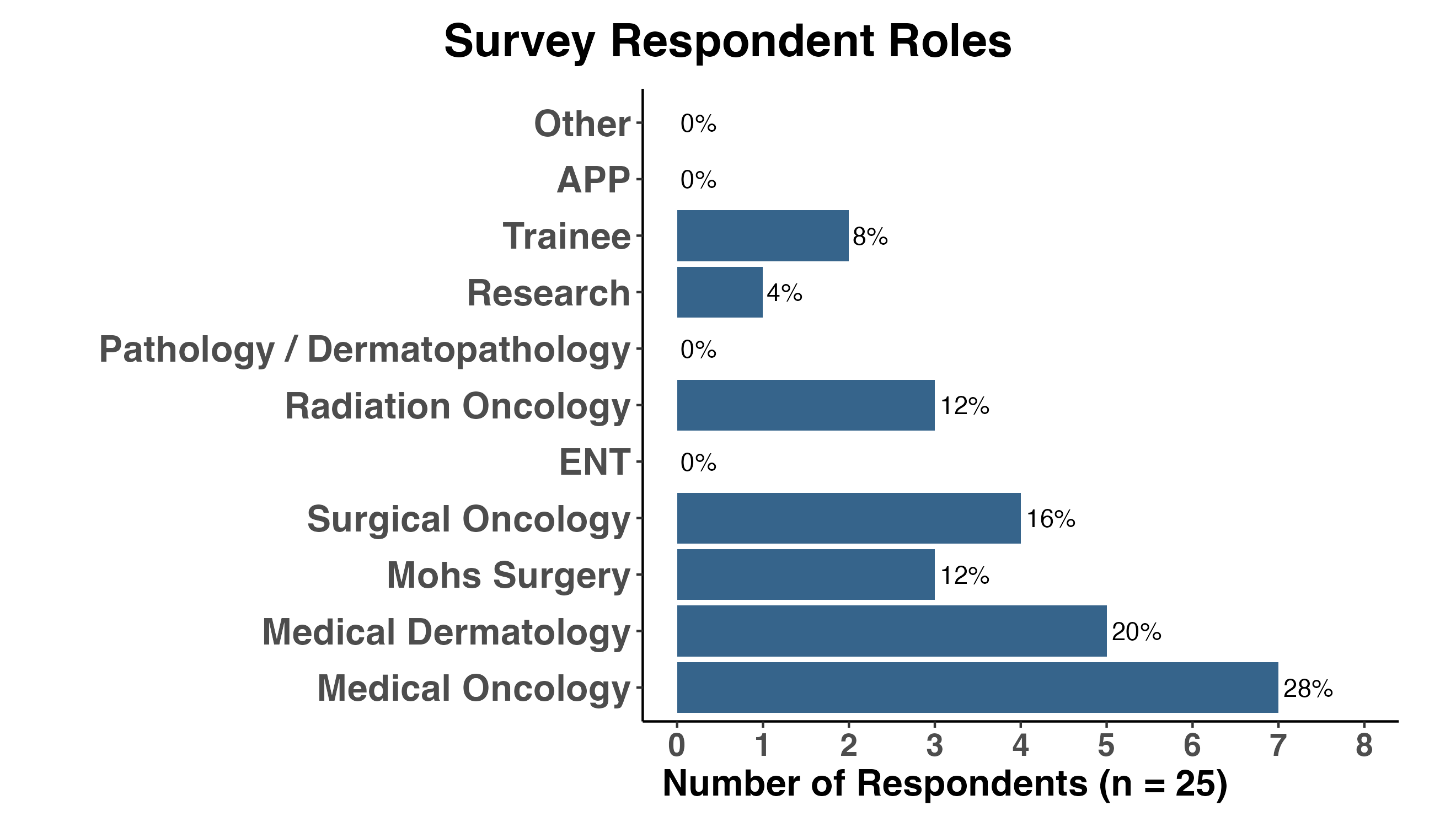
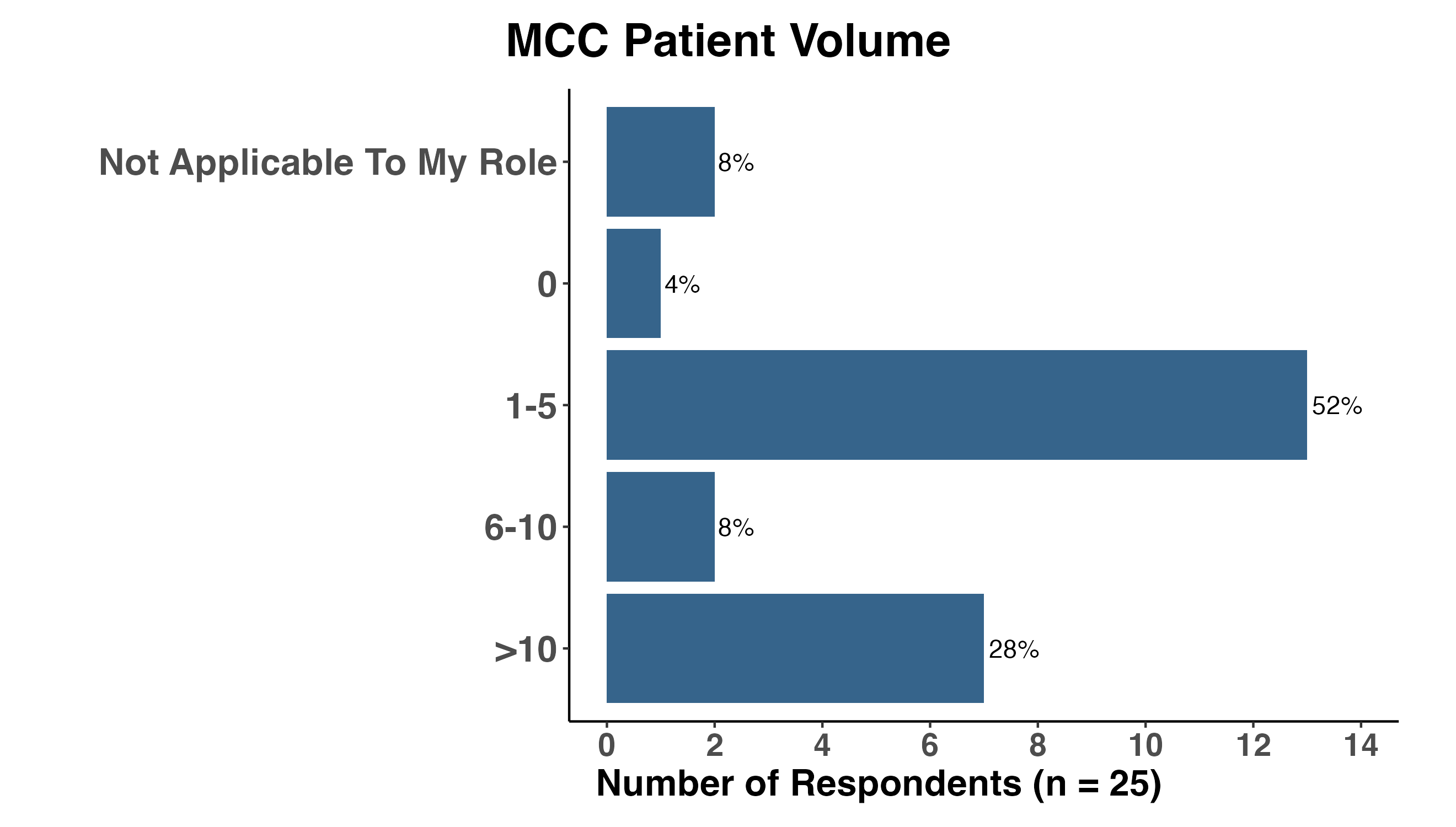
If the available evidence supported a single, compelling interpretation, one might expect practice patterns to converge. Instead, uncertainty surrounding local recurrence risk has translated into substantial variation in how clinicians estimate recurrence risk, recommend postoperative RT, and individualize treatment decisions. To better understand how clinicians interpret the current evidence, participants in the June 2026 Society of Cutaneous Oncology Journal Club completed a structured survey examining practice patterns, perceptions of recurrence risk, and attitudes toward postoperative RT.
NoteFigures 1–2. Survey respondent characteristics
Variation in Baseline Risk Estimates and Radiation Practice
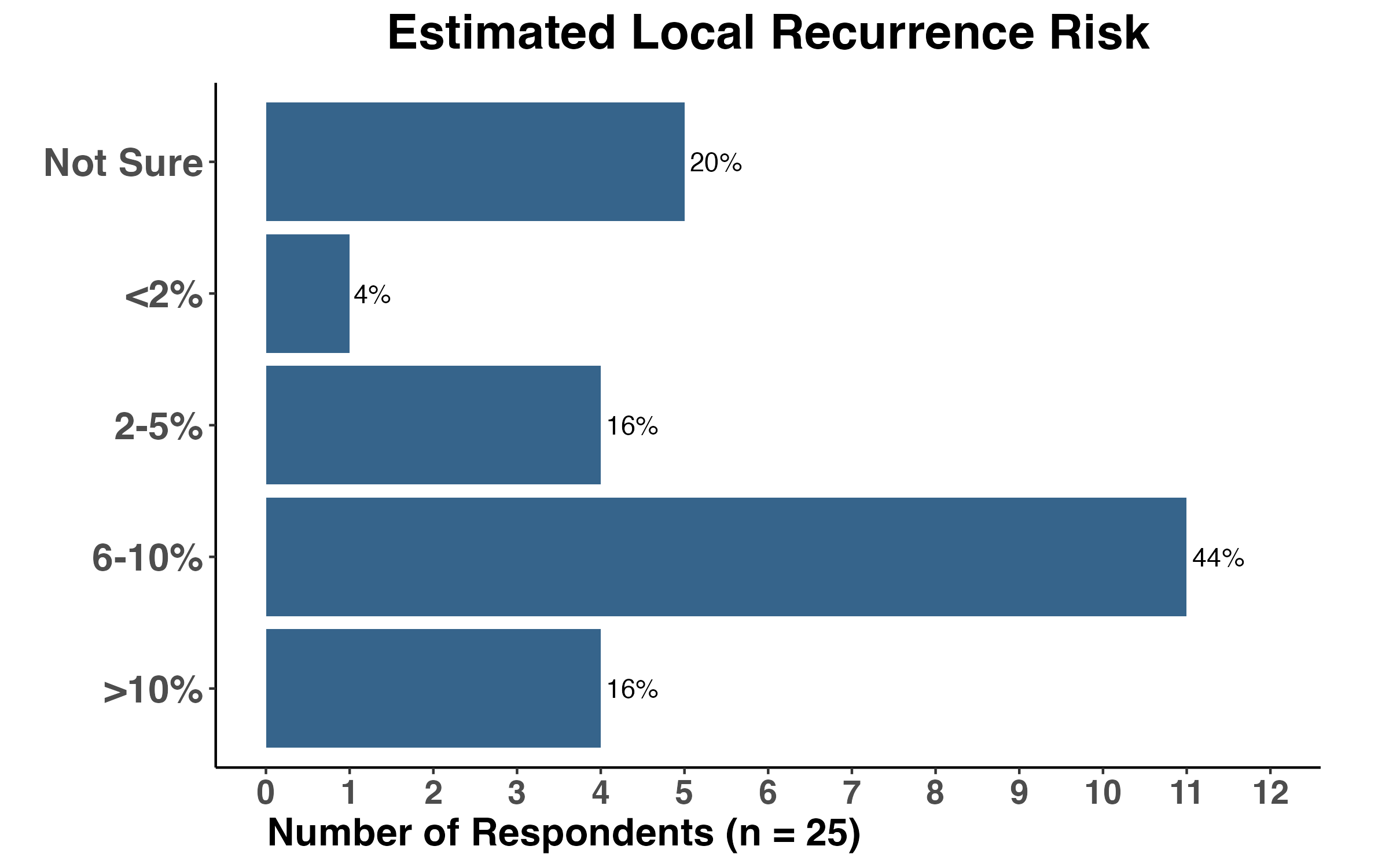
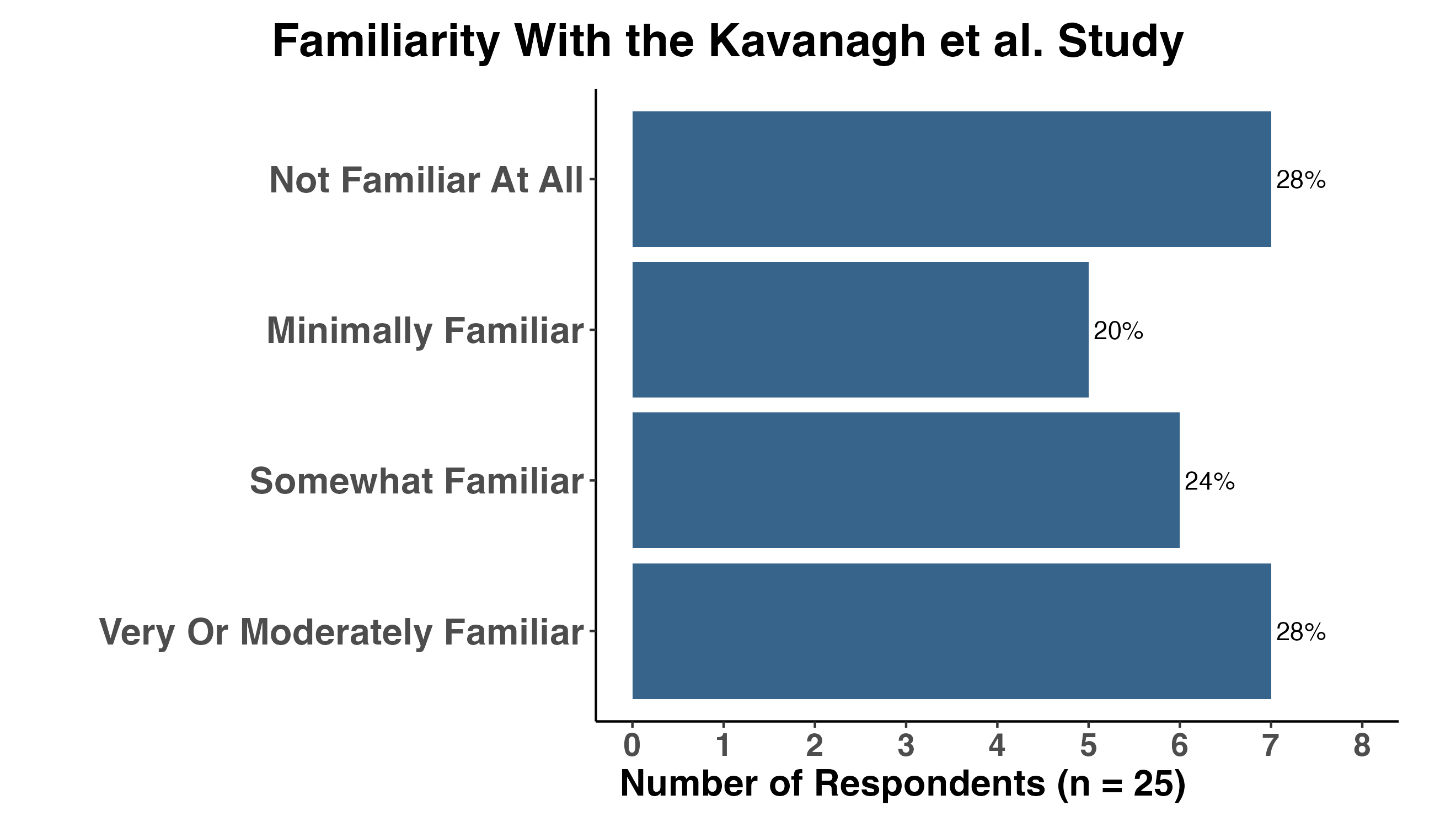
Despite broad agreement that local recurrence is an important outcome in MCC, survey responses revealed substantial variation in both perceived recurrence risk and approaches to postoperative RT (Figures 3–8). Baseline estimates of local recurrence after margin-negative excision ranged from less than 2% to greater than 10%, with most respondents estimating the risk to be between 6% and 10% (Figure 3). Notably, nearly one-half of respondents reported being minimally familiar or not familiar at all with the Kavanagh et al. study before the session (Figure 4), highlighting the limited dissemination of newer data specifically focused on local recurrence. Together, these findings suggest that variation in clinical practice reflects not simply differences in physician preference, but differences in how clinicians interpret an incomplete and evolving evidence base.
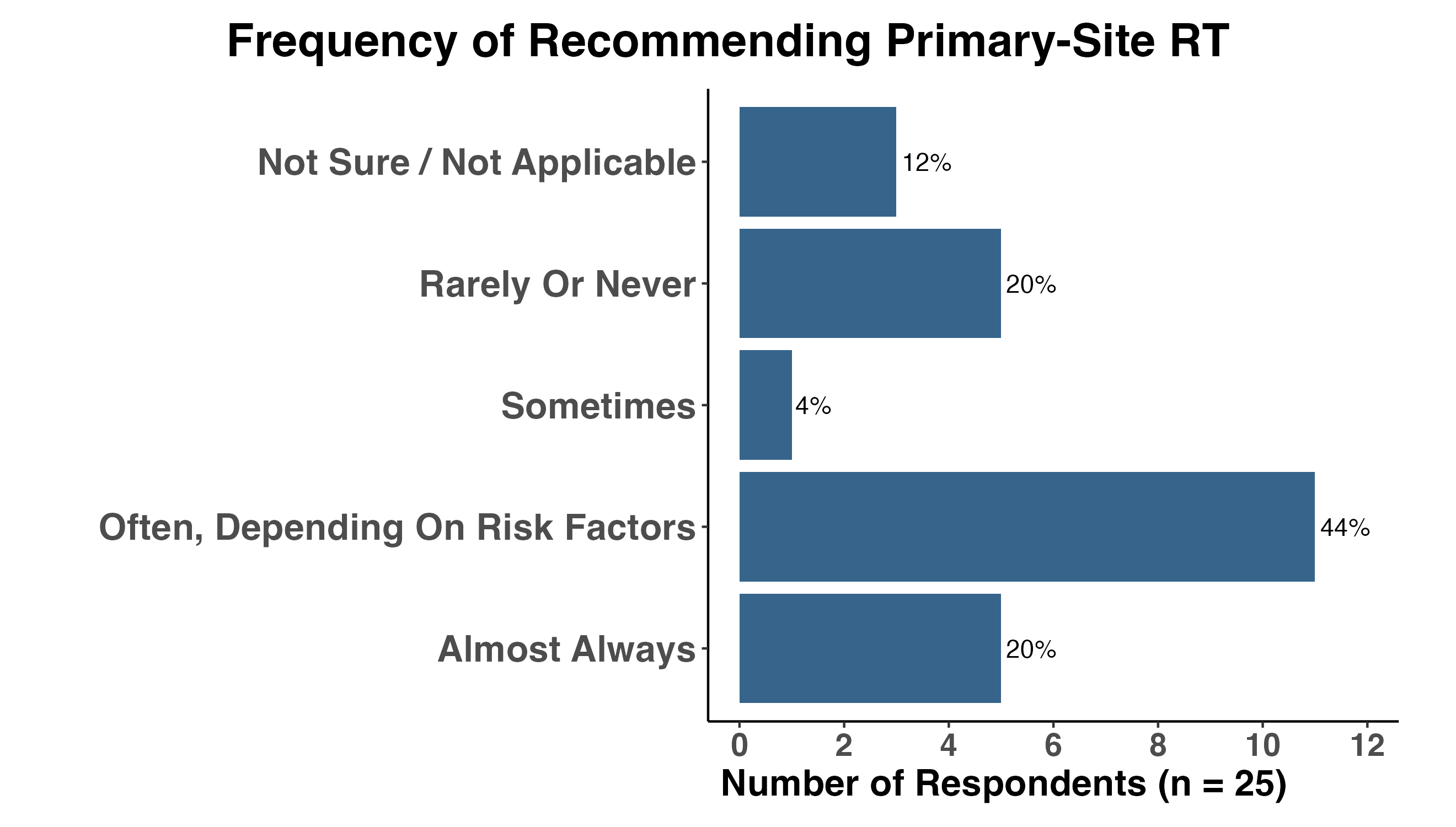
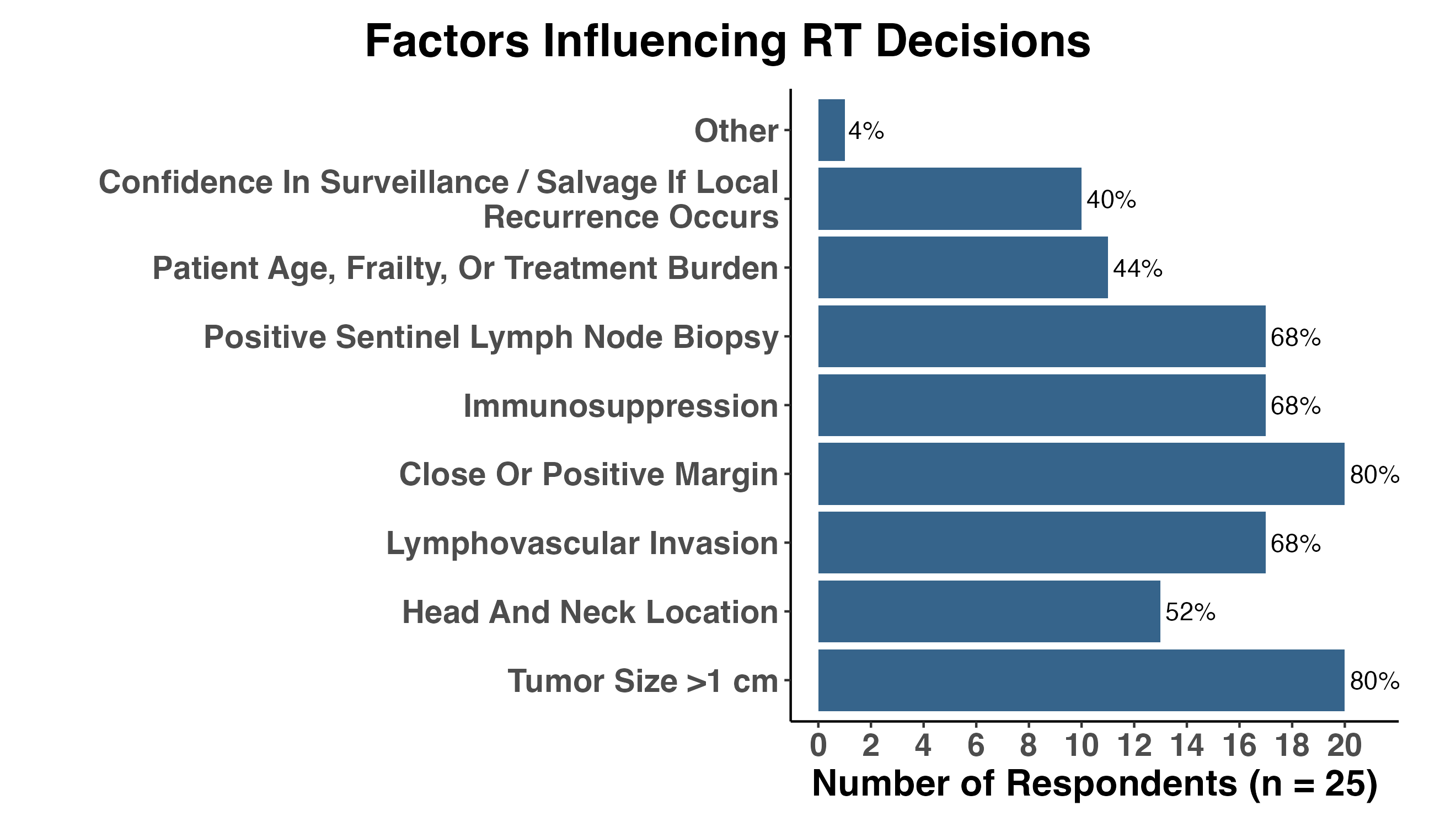
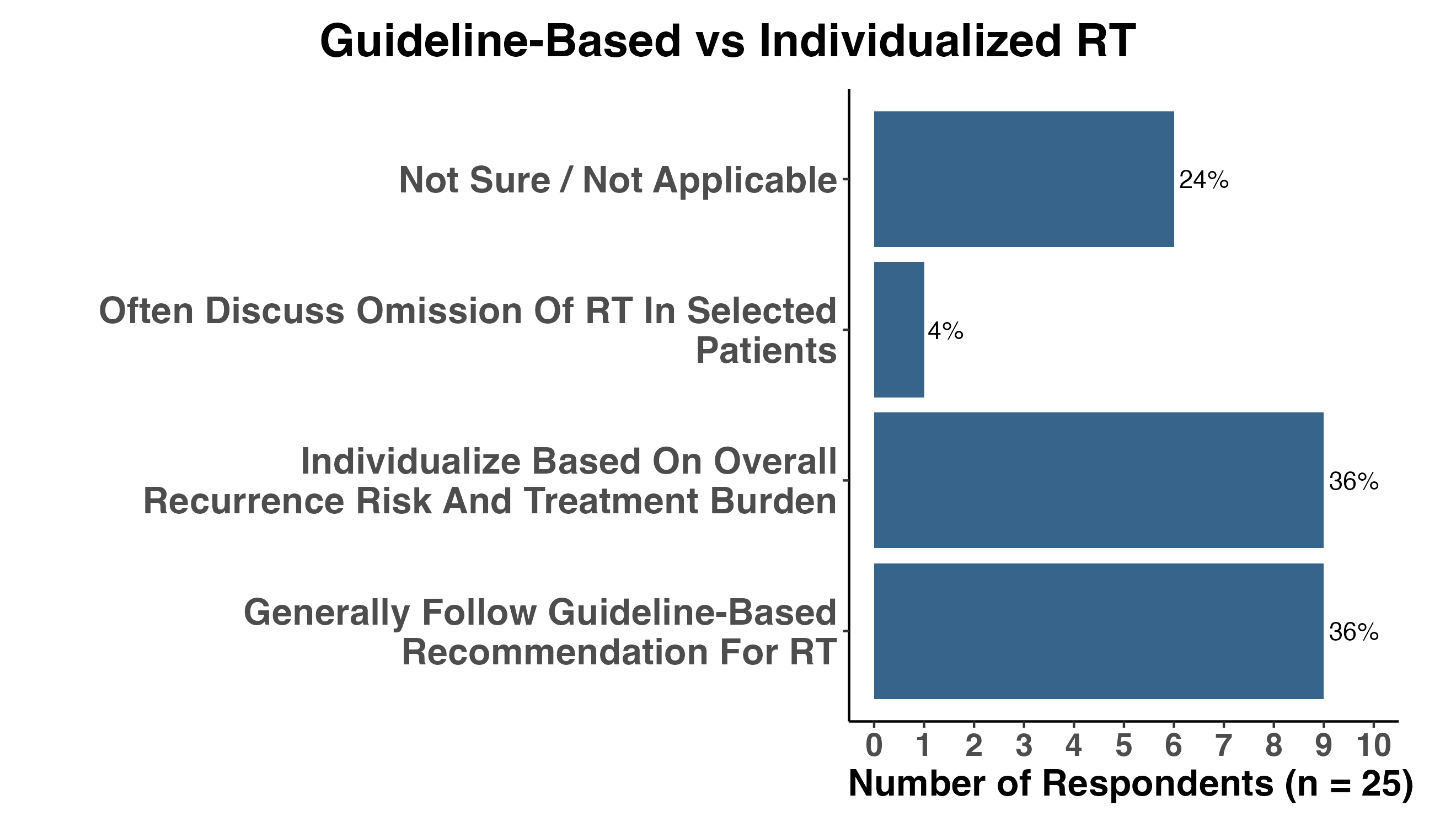
This uncertainty was also reflected in treatment recommendations. Equal proportions of respondents (20%) reported routinely recommending postoperative RT for nearly all patients or rarely recommending it at all, while the largest group (44%) indicated that their recommendations were individualized according to patient and tumor-specific risk factors (Figure 5). The factors most frequently influencing RT recommendations included tumor size greater than 1 cm, close or positive margins, lymphovascular invasion, immunosuppression, and positive sentinel lymph node biopsy findings (Figure 6). These factors closely mirror those incorporated into current NCCN recommendations, suggesting that variation in practice reflects not disregard for existing guidelines, but differences in how clinicians weigh the strength of the evidence supporting those risk factors and their implications for individual patients.
NoteFigures 3–8. Baseline beliefs and current practice patterns
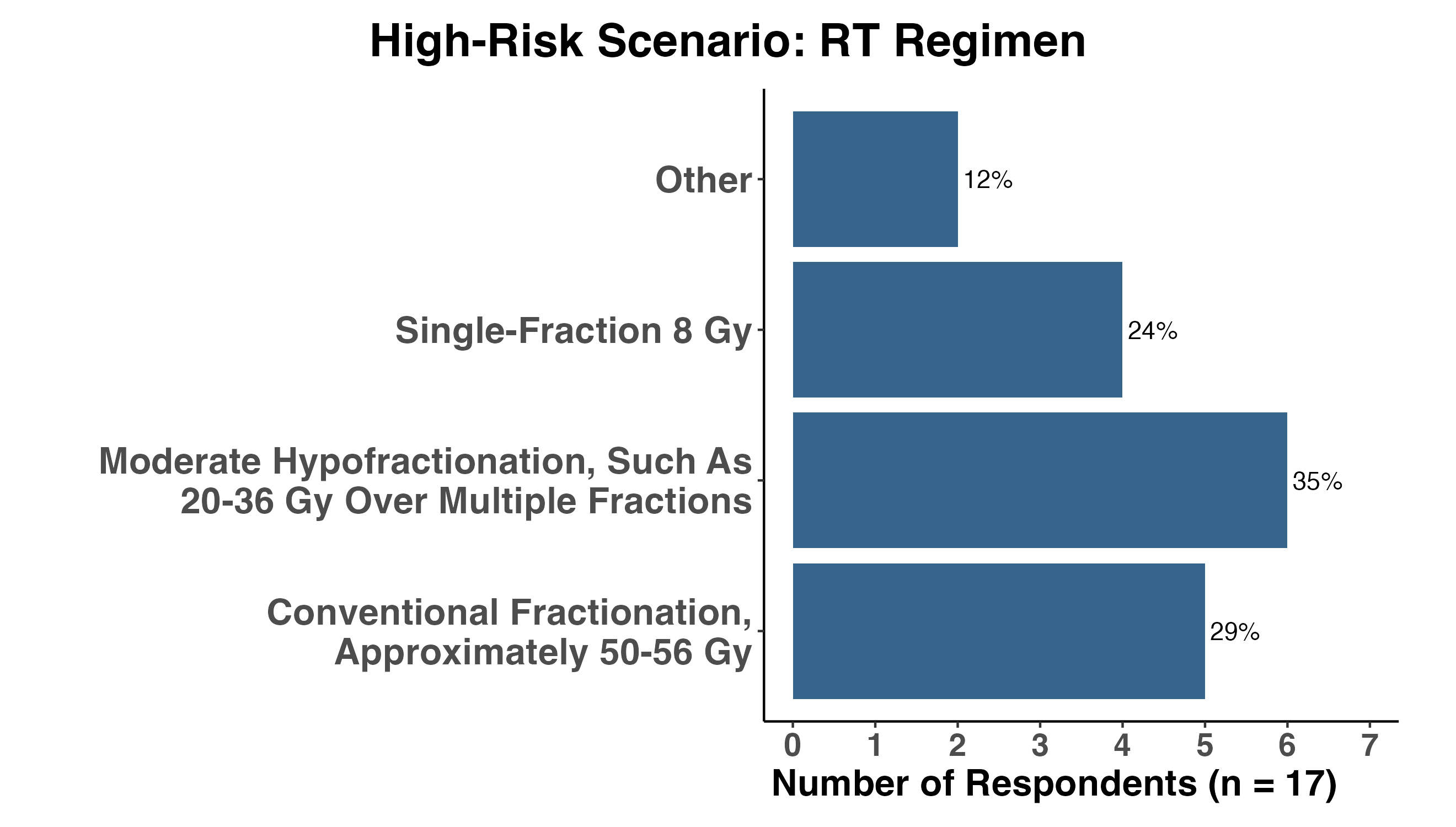
Evidence Thresholds and Areas of Equipoise
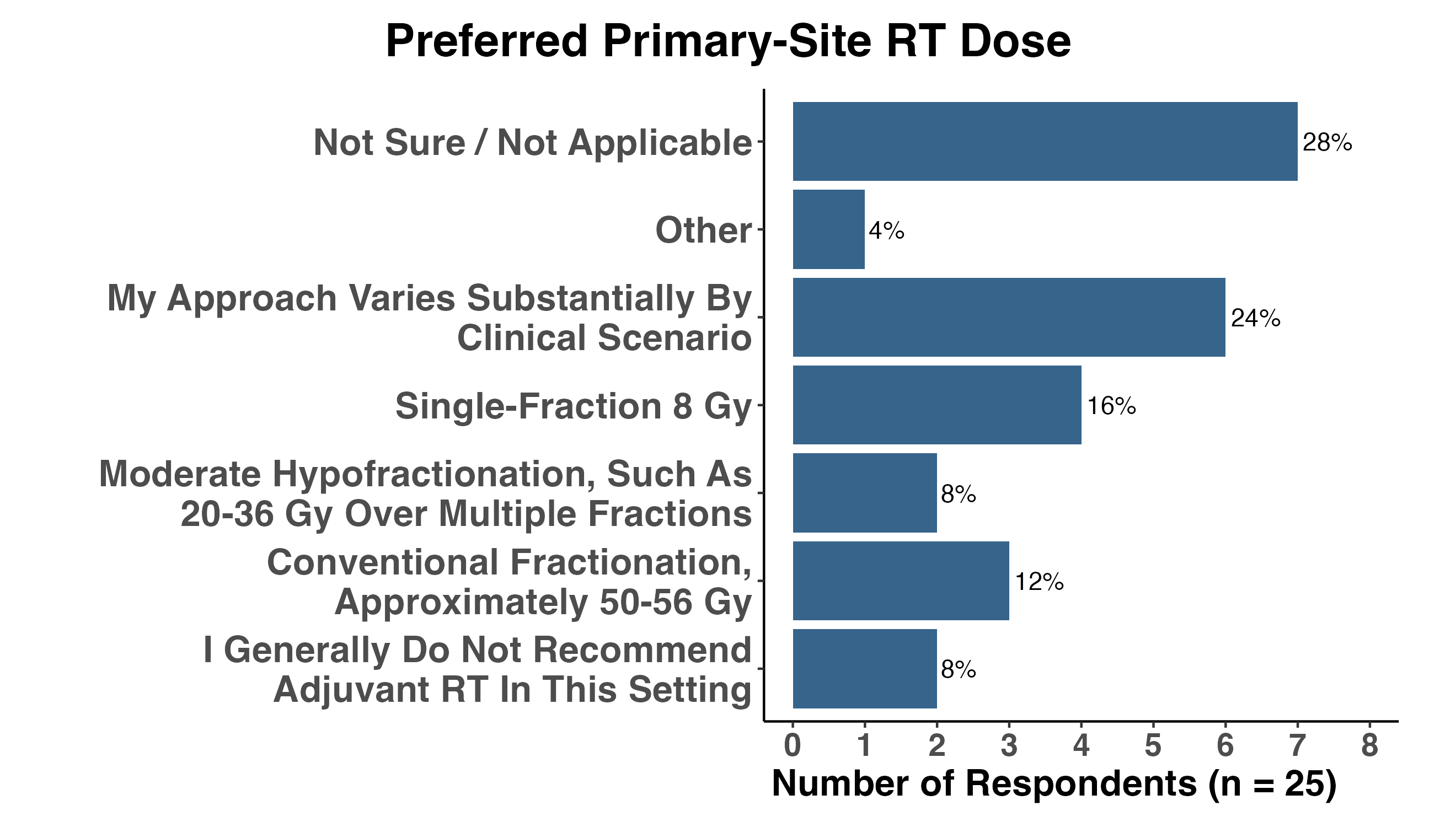
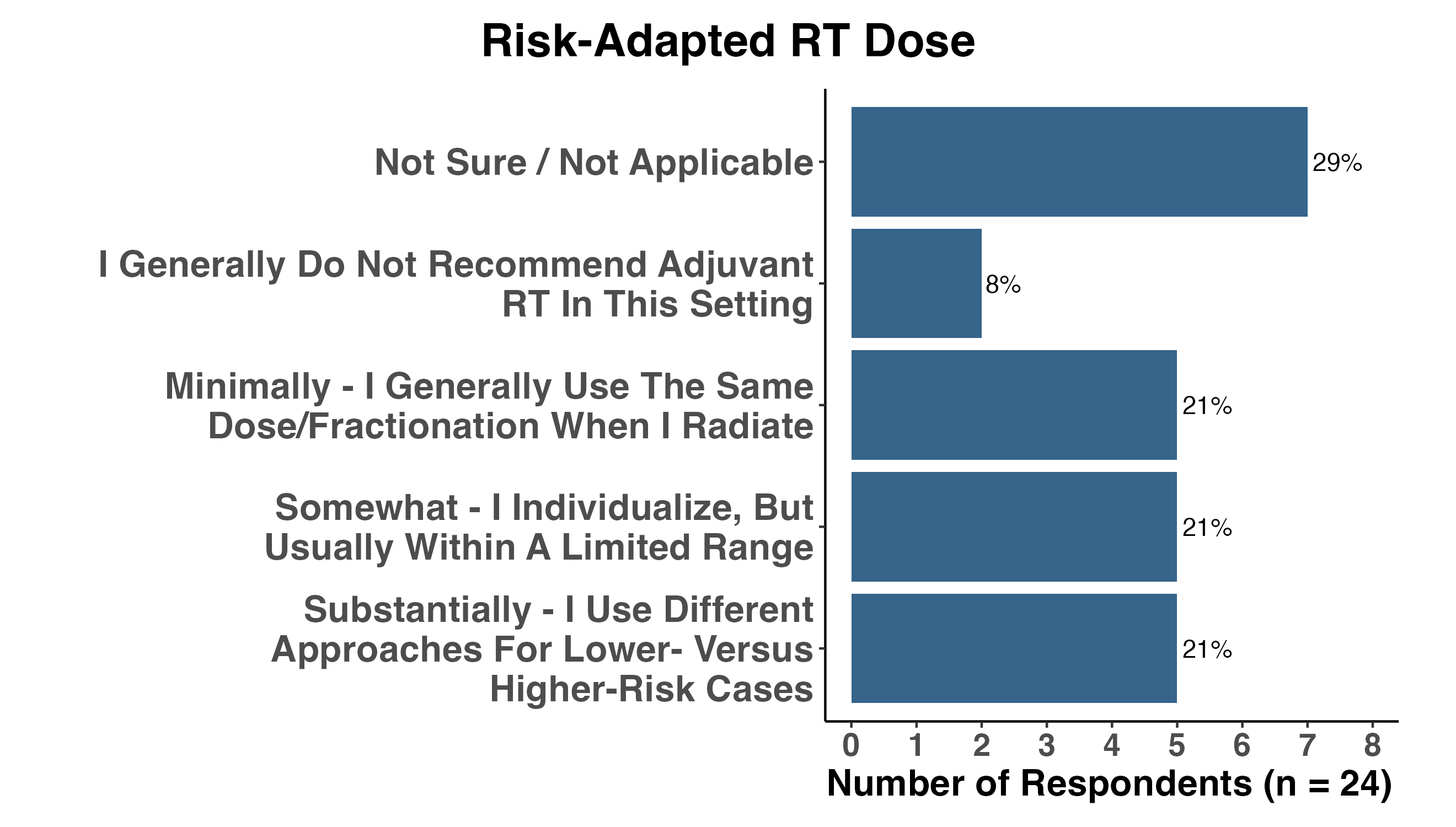
Survey responses also demonstrated that uncertainty in MCC management extends beyond the binary decision of whether postoperative RT should be recommended. Respondents reported a broad range of preferred dose and fractionation approaches, including conventional fractionation, moderate hypofractionation, and single-fraction 8 Gy, with substantial variation across clinical scenarios (Figures 9–10). Similarly, respondents differed in the degree to which they individualize dose and fractionation based on perceived recurrence risk, with equal proportions reporting minimal, somewhat, or substantial variation in approach.
Practice variation was therefore not limited to whether RT was used. Rather, uncertainty extended across multiple dimensions of care: baseline recurrence risk estimates, treatment thresholds, risk factors used in decision-making, dose/fractionation strategies, and assumptions about the detectability and salvageability of local recurrence. This pattern is consistent with meaningful clinical equipoise and supports the need for prospective evidence generation capable of informing not only whether RT should be used, but for whom, in what form, under what clinical circumstances, and with what expected benefit compared with observation and salvage therapy if local recurrence occurs.
NoteFigures 9–10. Variation in radiation dose and fractionation strategies
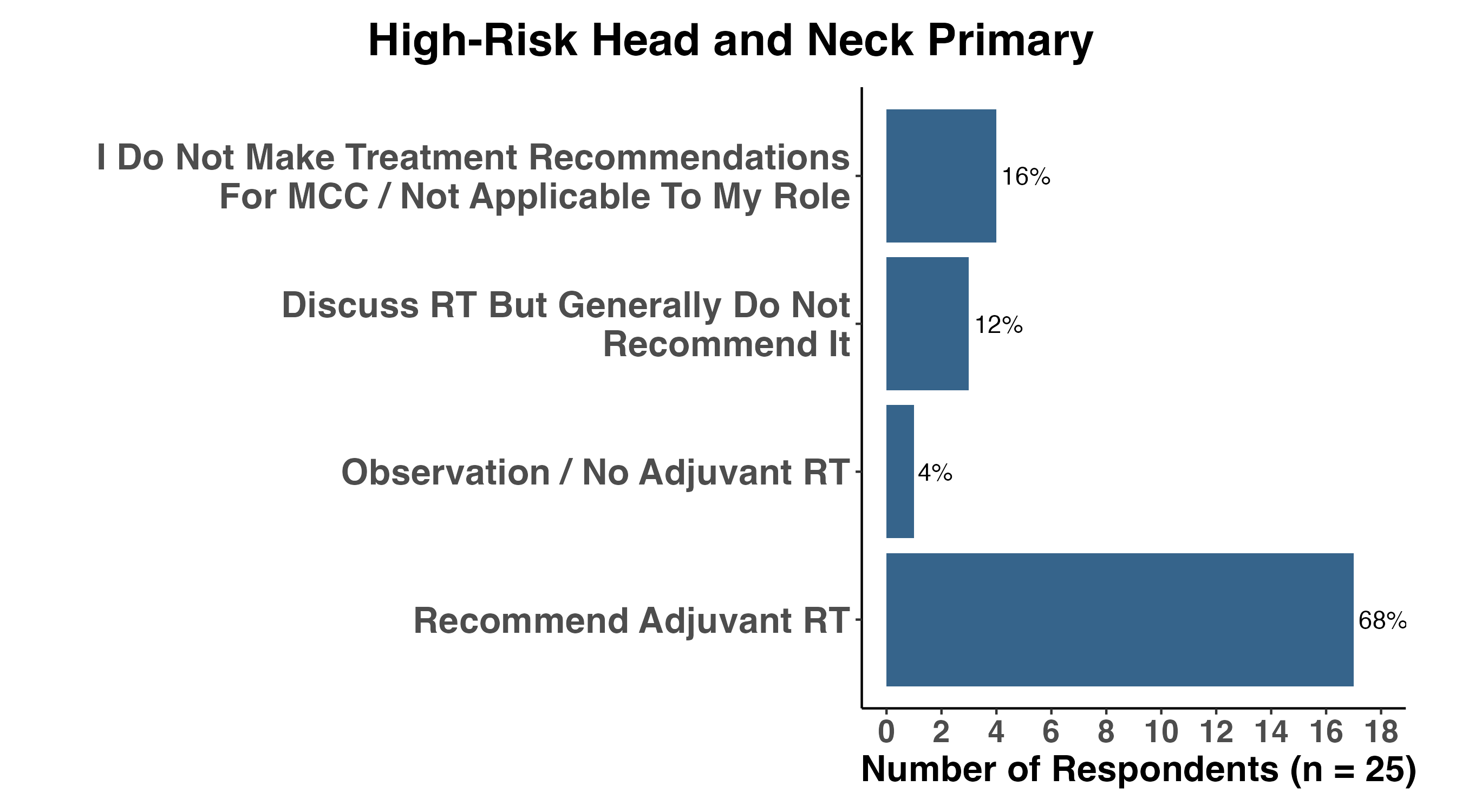
Clinical Scenarios Reveal Areas of Consensus and Disagreement
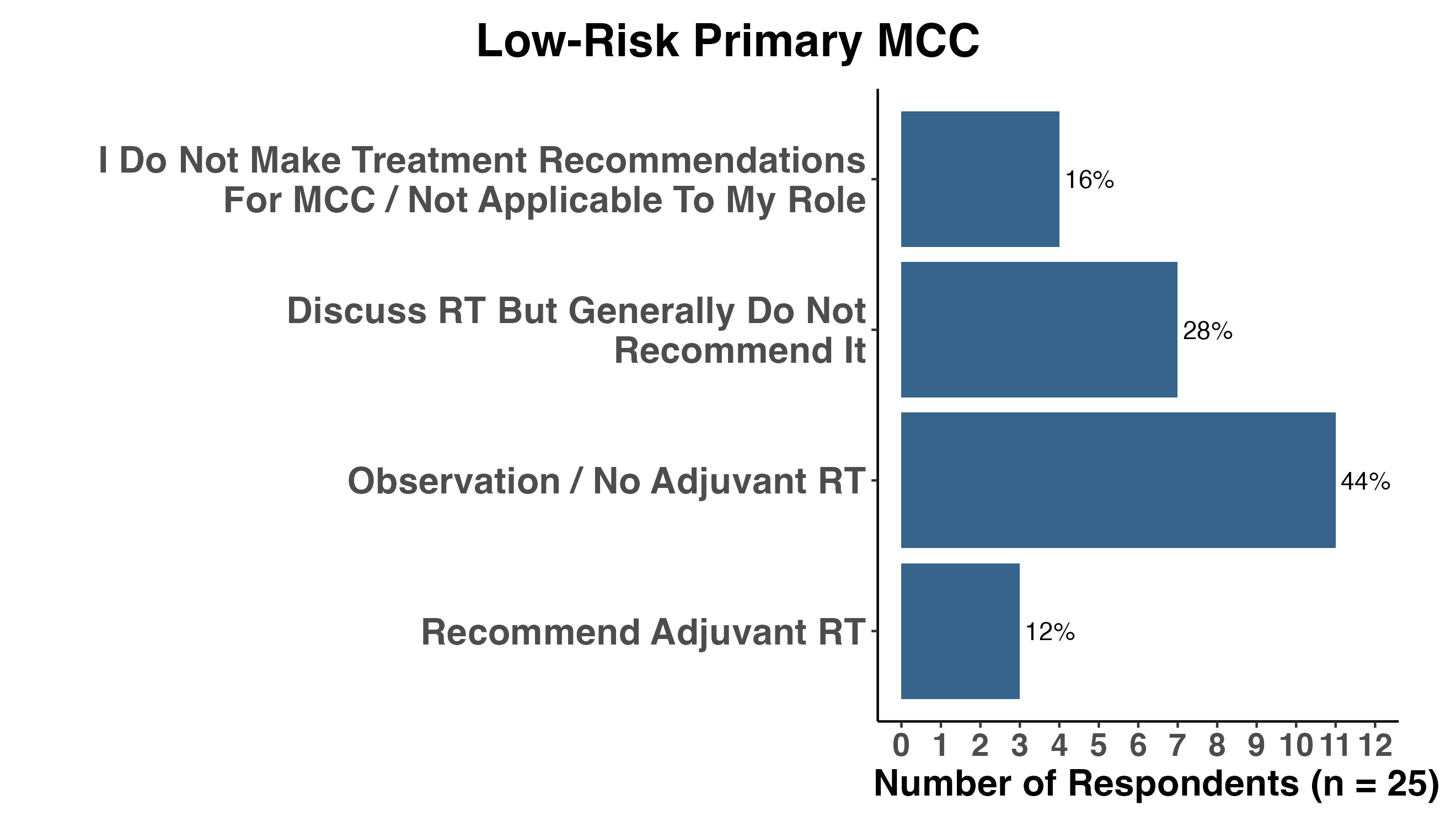
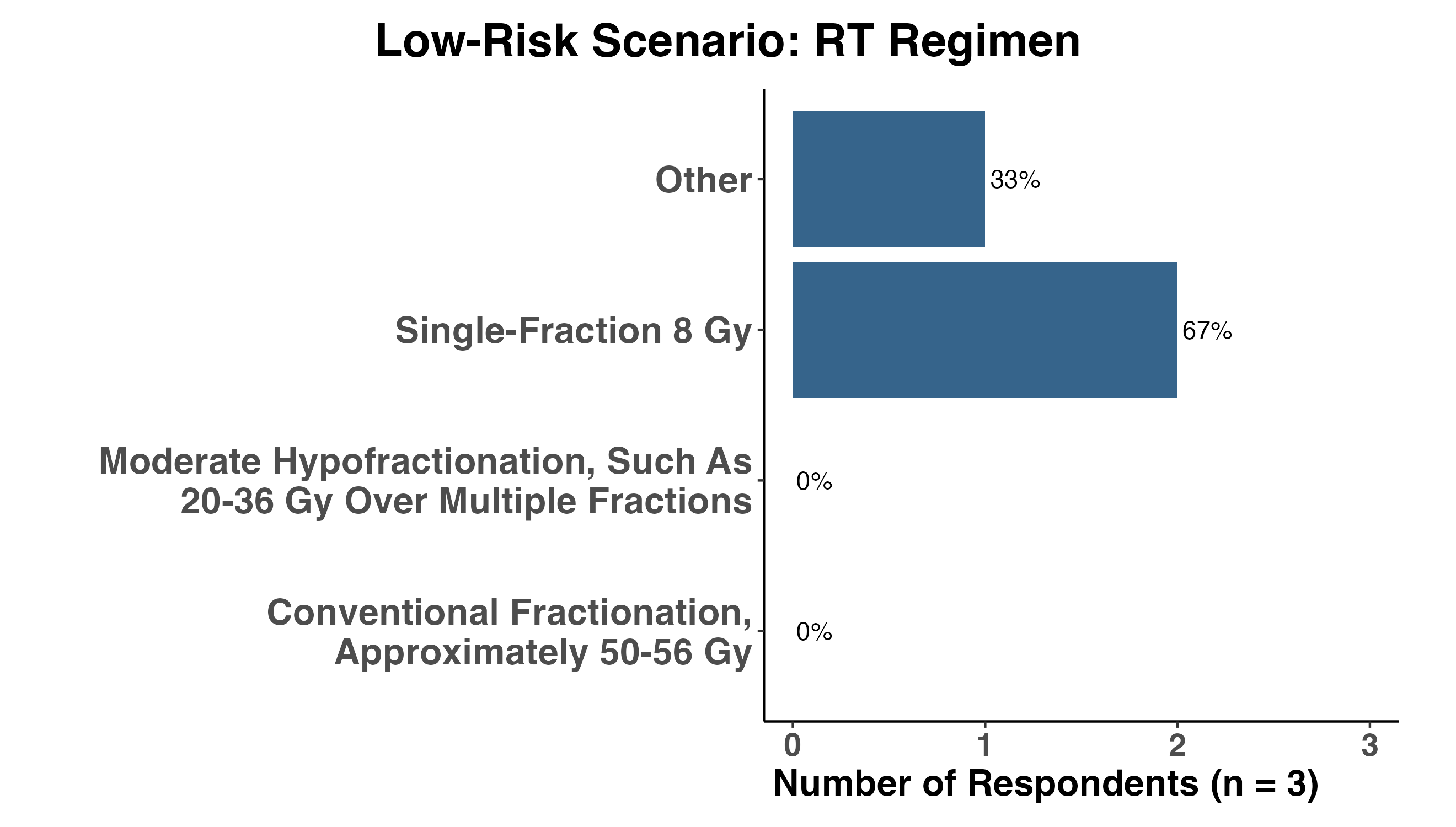
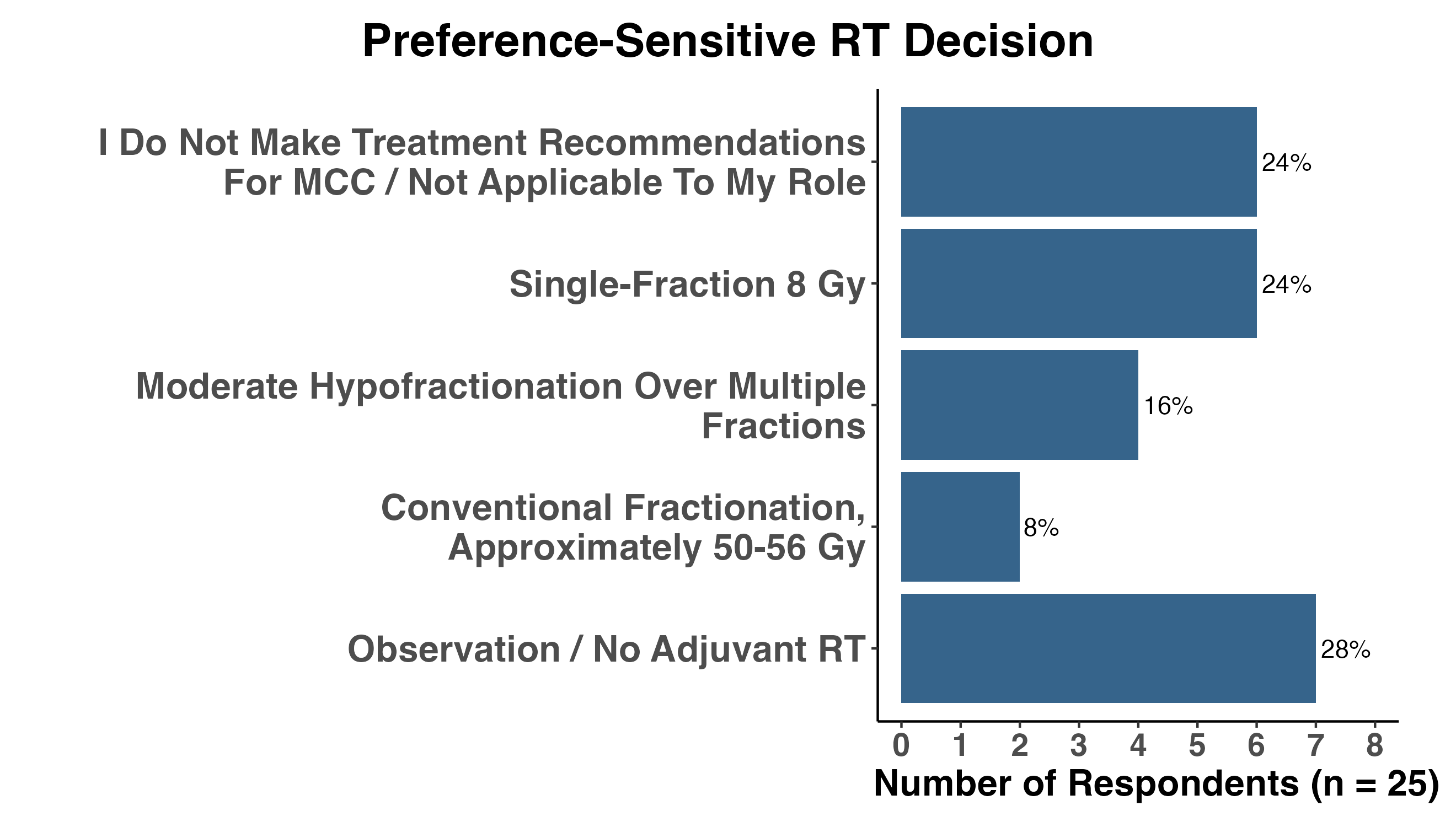
When respondents were presented with specific clinical scenarios, a consistent pattern emerged. Broad consensus was observed at the extremes of risk, whereas greater variation appeared in intermediate-risk settings where the balance between expected benefit and treatment burden was less certain (Figures 11–18). Observation was generally favored for a low-risk extremity primary lacking adverse features (Figure 11), whereas most respondents recommended RT for a patient with multiple guideline-defined risk factors, including head and neck location, lymphovascular invasion, close margins, and tumor size greater than 1 cm (Figure 13). These responses suggest that clinicians largely agree on which scenarios appear higher or lower risk, but differ in how they translate uncertain estimates of absolute benefit into treatment recommendations.
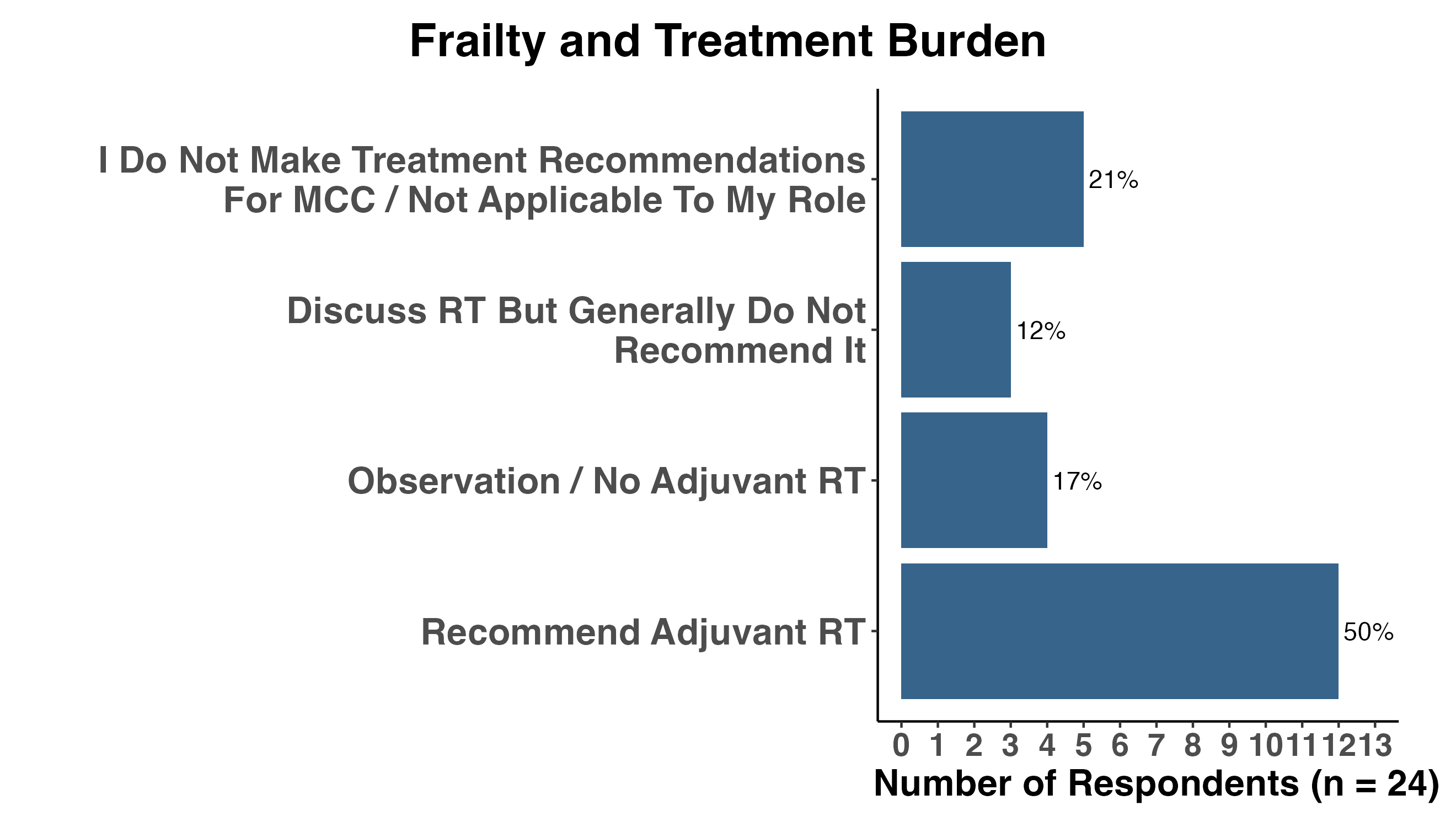
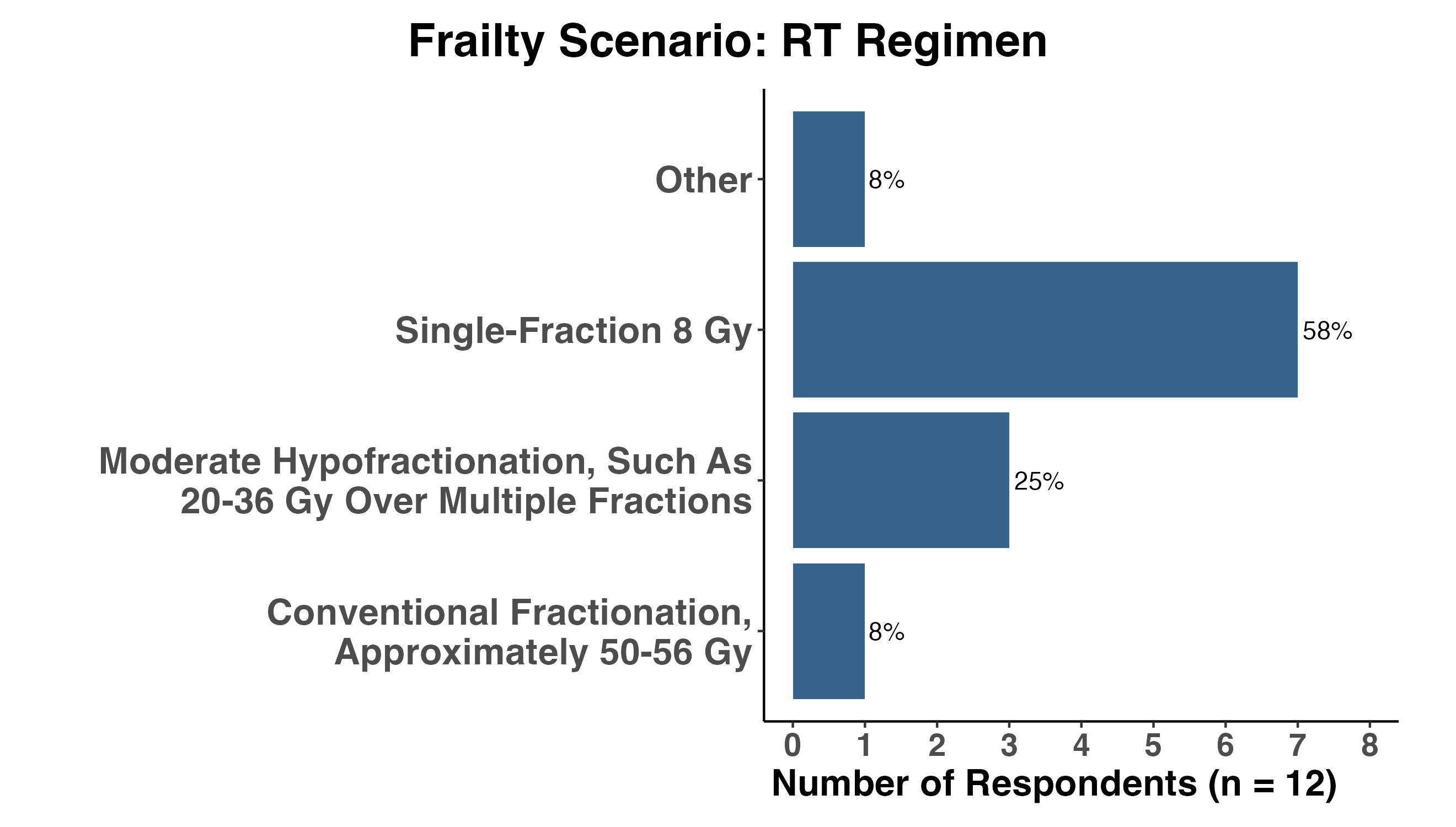
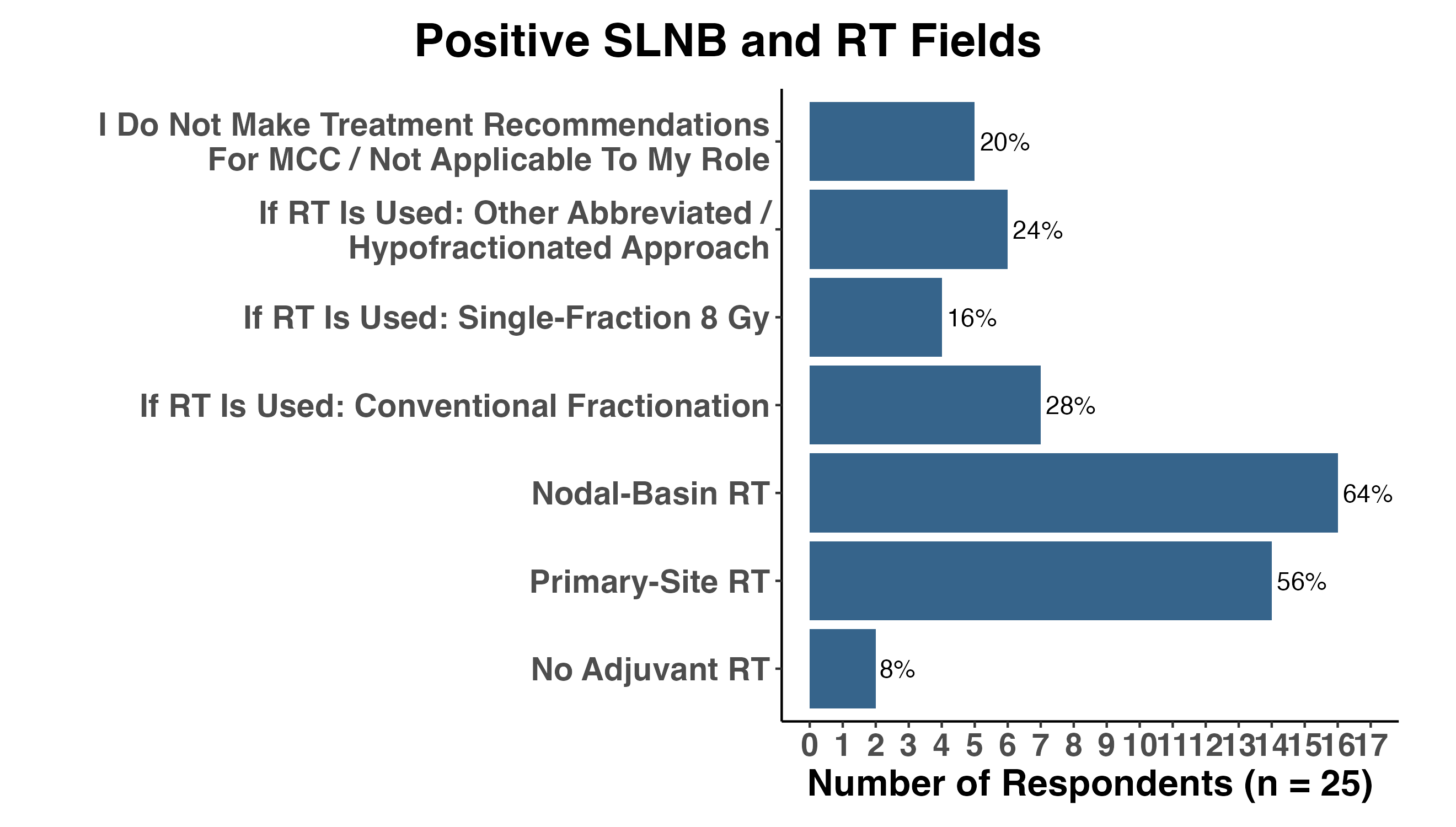
The scenarios also demonstrated that patient factors may influence the preferred approach to radiation delivery more than the binary decision to treat. In a scenario incorporating advanced age, frailty, travel distance, and treatment burden, most respondents still recommended RT (Figure 15), but single-fraction RT emerged as the dominant preferred regimen among those who would treat (Figure 16). Similarly, when a patient expressed a strong preference to minimize treatment burden, recommendations were distributed across observation and abbreviated or conventional RT approaches (Figure 17). Finally, in the setting of microscopic nodal involvement, respondents frequently selected nodal-basin RT and, in many cases, also selected RT to the local excision bed (Figure 18). This finding suggests that a positive SLNB often increases perceived treatment intensity and broadens consideration of RT fields, although whether microscopic nodal disease should influence treatment of the local excision bed remains a separate and unresolved question.
Taken together, these scenario-based responses suggest that practice variation in localized MCC is not random. Rather, clinicians appear to integrate tumor risk, anatomic site, nodal status, patient frailty, treatment burden, and feasibility of abbreviated radiation approaches. Future evidence generation should therefore capture not only recurrence outcomes, but also salvage treatment, disease-specific outcomes, and the patient- and clinician-level factors that shape treatment decisions. Such data are essential if future research is to improve decision-making rather than simply produce more precise recurrence estimates.
NoteFigures 11–18. Clinical scenario responses
Defining the Clinical Question
Although the Kavanagh study focused on local recurrence after complete surgical excision of primary MCC, the broader debate surrounding adjuvant RT may be driven as much by the questions being asked as by the available evidence. Clinicians may appear to disagree about the role of RT while, in reality, attempting to answer fundamentally different clinical questions. Disagreement may arise not only from how the available data are interpreted, but also from assumptions regarding baseline recurrence risk, the mechanisms by which RT might provide benefit, the clinical significance of the events being prevented, the effectiveness of salvage therapy, and the harms associated with treatment. Clarifying these questions is essential before considering what type of future evidence is needed—and whether additional retrospective studies are likely to resolve the controversy.
What Is the True Baseline Risk?
A natural instinct is to ask, “What is the true baseline risk of local recurrence?” Yet the available evidence suggests that this question may not have a single definitive answer. Among patients treated with margin-negative excision alone, Kavanagh et al. observed a 1-year local recurrence rate of just 1.8%, substantially lower than estimates reported in many historical series and lower than recurrence risks commonly cited during clinical decision-making1.
Interpretation of this estimate remains challenging. Approximately 12% of patients in the Kavanagh cohort received adjuvant RT, and these patients differed from those managed with surgery alone: they were younger, had larger tumors, more frequent LVI or tumor emboli, and a higher prevalence of NCCN-listed high-risk features, although they also had wider clinical margins1. These differences suggest nonrandom treatment selection, but they do not establish that the features prompting RT were independent predictors of local recurrence. Indeed, 75% of patients managed with surgery alone had at least one NCCN-listed high-risk feature, and the low number of local recurrence events precluded reliable identification of clinicopathologic predictors. As a result, the observed local recurrence rate among surgery-alone patients may not represent the risk that would have been observed in an entirely unselected population, but the Kavanagh data also challenge the assumption that currently used adverse features reliably discriminate patients at high risk for local recurrence.
A key area of uncertainty is whether the real-world risk of local recurrence is closer to 2%, as suggested by Kavanagh et al., or meaningfully higher in broader clinical practice. Several prior institutional and multicenter series report higher rates of recurrence or progression, but many were smaller, included mixed-treatment cohorts, used heterogeneous recurrence endpoints, or did not isolate local recurrence after margin-negative excision with the same methodological specificity. At the same time, framing the debate as a choice between 2% and 10% may oversimplify a more nuanced reality. The risk of local recurrence is unlikely to be a single fixed quantity applicable to all patients; rather, it almost certainly varies according to patient characteristics, tumor biology, treatment selection, and other measured and unmeasured factors. The more meaningful question may therefore be not whether one study has identified the “true” recurrence rate, but how uncertainty about baseline risk should influence clinical decision-making. Ultimately, the implications of this uncertainty depend not only on the absolute recurrence risk, but also on the expected benefit of RT, the effectiveness of salvage therapy, and the clinical consequences of the events being prevented.
What Does Primary-Site RT Prevent?
A central unresolved question is whether primary-site RT should be understood narrowly as an intervention to prevent local recurrence, or more broadly as a treatment that may sterilize residual microscopic dermal or lymphatic disease before it declares itself as in-transit, nodal, or distant progression.
The Kavanagh data most directly address the first question: whether complete excision without primary-site RT is followed by clinically consequential local failure. After negative-margin surgery, local recurrence was uncommon and occurred early. Among the eight patients who developed local recurrence, six had local recurrence alone, while two had local recurrence with simultaneous regional and distant metastatic disease. All six patients with isolated local recurrence received additional local therapy, achieved durable local control, and none subsequently died of MCC. By contrast, the two patients with local recurrence accompanied by synchronous regional and distant metastases progressed rapidly despite systemic therapy, a pattern the authors interpreted as more consistent with aggressive disease biology than failure of initial local treatment. Thus, within the limits of an analysis focused on local recurrence, these data provide little evidence that omission of primary-site RT commonly leads to unsalvageable local failure or to a substantial burden of metastatic relapse clearly arising from uncontrolled local disease.
The small number of recurrence events limits definitive conclusions regarding whether RT might prevent some events beyond local recurrence alone. Nevertheless, the available data more strongly support a model in which most isolated local recurrences behave as local events that can be effectively salvaged, rather than as precursors of later regional or distant progression. This distinction matters. If primary-site RT primarily prevents rare and salvageable local recurrences, then many patients may receive treatment without meaningful clinical benefit. If, instead, RT interrupts a broader pathway of locoregional or systemic progression, then local recurrence alone may underestimate its clinical value.
At present, the Kavanagh data provide stronger support for the former hypothesis than the latter, while also underscoring the need for future studies to capture not only whether recurrence occurs, but what type of recurrence occurs, how it is treated, and whether it affects disease-specific outcomes.
How Salvageable Is the Event Being Prevented?
The clinical value of adjuvant RT depends not only on how often recurrence occurs, but also on what happens when recurrence develops. A local recurrence that can be detected early and successfully salvaged through surgery, RT, or systemic therapy carries different implications than a recurrence that serves as a precursor to uncontrolled regional or distant dissemination.
An implicit assumption in many discussions of local recurrence is that all recurrences carry equivalent clinical importance. In practice, however, the consequences of recurrence may vary substantially according to timing, location, patient fitness, and the availability of effective salvage options. This consideration is particularly relevant in MCC, where advances in immune checkpoint blockade have altered the therapeutic landscape and improved outcomes for many patients with recurrent disease.
The Kavanagh experience is notable in this regard. Among patients with isolated local recurrence, durable disease control was achieved with additional local therapy, and none subsequently died of MCC. In contrast, the two patients who developed local recurrence together with regional and distant metastatic disease experienced poor outcomes despite systemic therapy. This pattern suggests that the clinical significance of recurrence may depend less on the presence of a local recurrence itself and more on the biological context in which it occurs.
If most isolated local recurrences remain highly salvageable, then the threshold for recommending routine adjuvant RT may be higher. Conversely, if local recurrence occurs in association with regional or distant progression, it is important to distinguish whether the local event is a cause of subsequent spread, a marker of aggressive tumor biology, or one manifestation of disease that was already systemic. These scenarios have different implications for adjuvant RT. Preventing a local recurrence would have broader clinical value only if that event would otherwise contribute meaningfully to subsequent progression. If, instead, local recurrence occurs simultaneously with regional or distant disease, then treatment of the primary site addresses only one component of a more aggressive biological process. Thus, the value of adjuvant RT cannot be judged solely by counting recurrences. It must also be judged by the clinical significance of the events prevented, the effectiveness of salvage therapy, and the extent to which prevention of local recurrence changes disease-specific outcomes.
What Are the Harms of Treatment?
Discussions regarding adjuvant RT often focus on recurrence prevention while devoting comparatively less attention to treatment-related harms. Yet the risk-benefit calculation depends critically on both sides of the equation.
Conventional postoperative RT may be associated with acute toxicity, fibrosis, lymphedema, alopecia, wound-healing complications, treatment burden, financial cost, and, in rare circumstances, serious long-term sequelae. These considerations become increasingly important when the anticipated absolute reduction in recurrence risk is small. Even if RT is highly effective at preventing local recurrence, the clinical value of treatment depends on whether the expected benefit outweighs these competing harms.
Importantly, RT should not be viewed as a single intervention. Contemporary practice encompasses a spectrum of approaches ranging from conventional fractionation to abbreviated hypofractionated regimens and single-fraction RT. Survey responses demonstrated substantial variation in preferred dose and fractionation schedules, particularly in scenarios involving advanced age, frailty, or logistical barriers to treatment. These findings suggest that the debate may not simply be whether RT should be delivered, but how it should be delivered and at what cost in terms of patient burden.
Taken together, these considerations suggest that disagreements regarding adjuvant RT in localized MCC extend well beyond estimates of local recurrence risk alone. Clinicians may arrive at different treatment recommendations because they hold different assumptions regarding baseline risk, treatment effect, salvageability, and toxicity. These questions are closely intertwined, and each may require different forms of evidence to answer. The challenge is therefore not simply to generate more data, but to generate evidence that meaningfully informs clinical decision-making.
Are We Asking More of Retrospective Studies Than They Can Answer?
Taken together, these considerations suggest that many of the questions surrounding adjuvant RT in localized MCC may be difficult to answer using conventional retrospective analyses alone. Decisions regarding RT are influenced by tumor characteristics, surgical technique, patient factors, physician judgment, and institutional practice patterns, creating substantial potential for confounding by indicationa. At the same time, local recurrence remains a relatively uncommon event, limiting statistical power even in large institutional series.
Notea Confounding by Indication
Confounding by indication occurs when the reason a treatment is given is also related to the outcome being studied. In the context of adjuvant RT for MCC, patients selected for radiation may have larger tumors, closer margins, lymphovascular invasion, head and neck primary sites, immunosuppression, or other features that make recurrence more likely.
As a result, comparing patients who received RT with those who did not can be misleading. If the RT group has similar outcomes despite having higher-risk disease, RT may be beneficial. If the RT group has worse outcomes, this may reflect baseline risk rather than harm from radiation. Statistical adjustment can reduce measured confounding, but uncertainty remains whenever treatment selection is influenced by clinical judgment or other factors that are incompletely measured.
Retrospective studies remain indispensable for understanding the natural history of disease, describing patterns of care, estimating recurrence risk, and generating clinically important hypotheses. Their principal limitation is not that they are retrospective, but that they are often asked to answer causal questions for which they were not designed. This distinction is particularly important when the objective shifts from describing recurrence to estimating which patients derive meaningful net benefit from treatment. Such questions require consideration of treatment selection, competing risks, and patient-centered outcomes—including toxicity, functional outcomes, cosmetic outcomes, travel burden, financial toxicity, and quality of life—which are often incompletely captured in retrospective datasets.
The rarity of local recurrence further compounds these challenges. If the true recurrence risk after margin-negative excision is approximately 2–8%, even large institutional cohorts may contain relatively few events. Small differences in event counts can therefore produce meaningfully different recurrence estimates, while subgroup analyses may remain unstable despite seemingly large sample sizes. Consequently, simply accumulating larger retrospective cohorts may not fully resolve the underlying uncertainty.
Viewed through this lens, the central challenge is no longer simply obtaining a more precise estimate of recurrence risk. Rather, it is developing an evidence-generation framework capable of estimating individualized treatment benefit while explicitly accounting for treatment selection, competing risks, patient-centered outcomes, and uncertainty. Addressing that challenge will likely require complementary approaches, including prospective data collection, harmonized analyses of existing multicenter cohorts, and modern causal and probabilistic methods capable of estimating treatment benefit under uncertainty. The goal is not to replace retrospective research, but to integrate multiple sources of evidence in a framework that supports better clinical decision-making.
What Should Future Evidence Generation Look Like?
The limitations of the existing evidence base do not diminish the importance of the clinical question. Rather, they clarify how future evidence generation should be designed. The central limitation is not simply that many studies are retrospective. It is that much of the available evidence comes from administrative datasets or retrospective institutional series in which treatment rationale, recurrence definitions, radiation fields and fractionation, salvage treatment, toxicity, treatment burden, patient preferences, and disease-specific outcomes are incompletely or inconsistently captured.
If the central goal is to identify which patients derive meaningful benefit from adjuvant primary-site RT, then future studies must capture more than whether recurrence occurs. They must also define baseline risk, treatment strategy, recurrence pattern, salvageability, toxicity, treatment burden, patient preferences, and the clinical rationale underlying treatment selection.
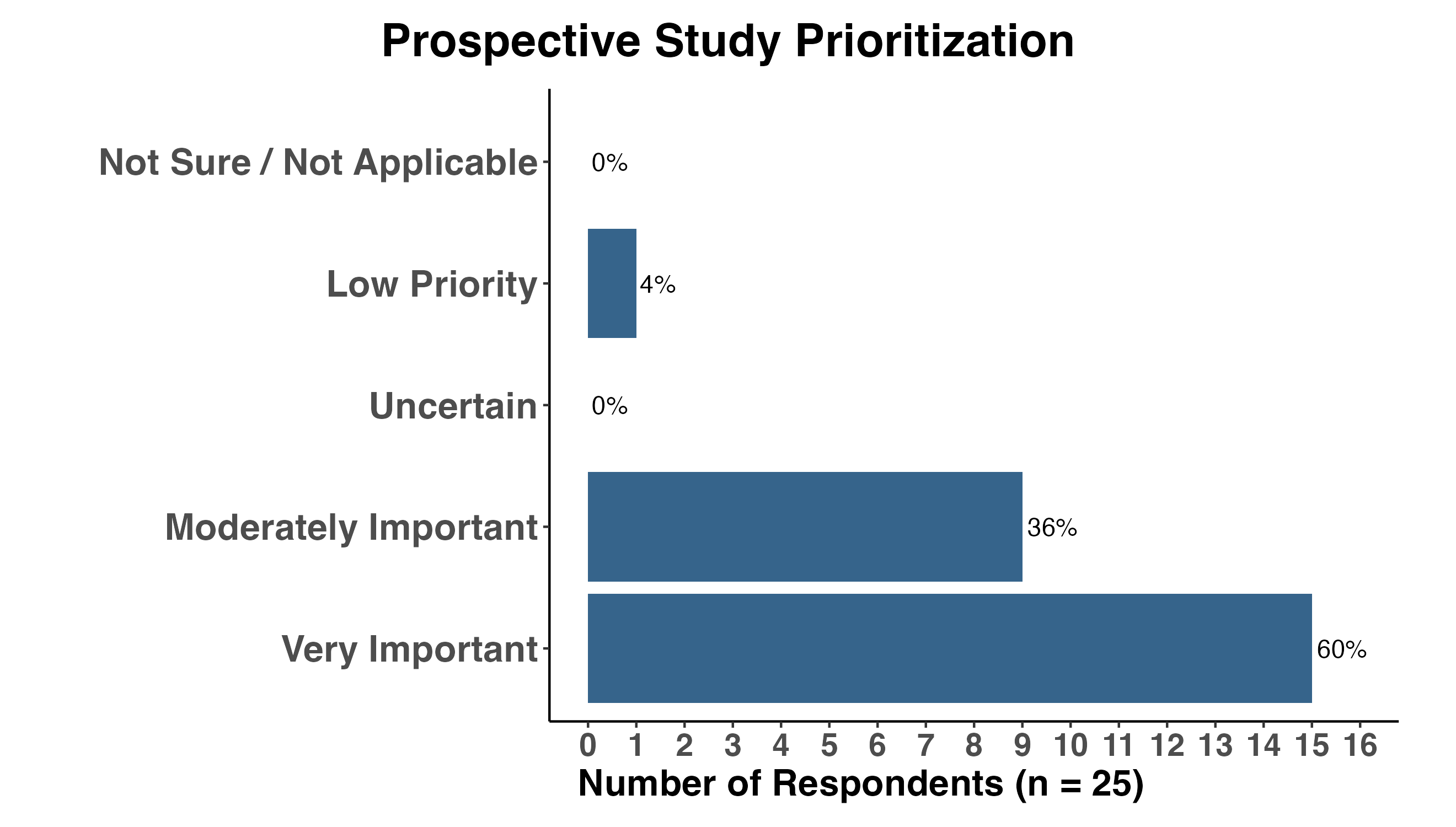
Survey responses supported the need for more structured multi-institutional evidence generation. Almost all respondents rated a prospective multicenter study of radiation after surgical excision of MCC as either very important or moderately important (Figure 19). This finding suggests that, despite differences in current practice, there is broad agreement that the existing evidence base remains insufficient to guide patient selection and treatment approach. Importantly, such a study should not simply catalogue whether adjuvant RT was used. Its highest value would be to more clearly define the natural history of local recurrence after complete excision, using standardized recurrence definitions, physician-curated event review, detailed treatment information, salvage treatment data, and disease-specific outcomes. In this respect, the Kavanagh study provides a useful methodological template: future datasets should seek to replicate, refute, or refine its findings across institutions and practice settings.
NoteFigure 19. Priority of prospective evidence generation
Prospective evidence generation should not be equated with the feasibility of a conventional randomized trial. A randomized trial would provide the cleanest estimate of treatment effect, but feasibility may be limited by the rarity of MCC, low local recurrence event rates, cost, heterogeneity in radiation approaches, and the need for genuine clinician and patient equipoise. The Journal Club discussion highlighted this challenge clearly: some clinicians favor adjuvant RT for nearly all patients with localized MCC, whereas others use it rarely or selectively. Conversely, an unstructured registry may be easier to implement but risks reproducing many of the same interpretive limitations that affect existing retrospective studies. The goal, therefore, is not to identify a single ideal study design, but to build an evidence-generation strategy capable of answering clinically meaningful questions despite the practical constraints of studying a rare cancer.
The most useful approach may lie between these extremes: a highly curated, multi-institutional observational effort, ideally prospective in design but also capable of incorporating protocolized retrospective case capture when key data elements can be reliably abstracted. Such efforts are feasible when organized around prespecified data elements, standardized definitions, transparent governance, equitable academic credit, and a shared commitment to data quality. A study designed in this manner would standardize recurrence definitions, capture the clinical rationale for treatment decisions, characterize radiation fields and fractionation in detail, record toxicity and patient-centered outcomes, and include salvage treatment and disease-specific outcomes as core endpoints. It should also be designed from the outset to support causal inference and hierarchical probabilistic modeling. Rather than asking whether retrospective or prospective evidence is inherently superior, this framework recognizes that rigorous science comes from combining complementary sources of evidence within a principled analytic approach.
Why Causal Inference Matters
A central challenge in studying adjuvant RT is that treatment is not assigned randomly. Clinicians selectively recommend RT to patients perceived to be at higher risk based on tumor size, lymphovascular invasion, immunosuppression, margin status, surgical technique, anatomic location, nodal status, frailty, and provider or institutional practice patterns. Consequently, treatment assignment itself contains information about recurrence risk.
Traditional analyses often compare outcomes among patients who received RT with those who did not. The difficulty is that these groups are often fundamentally different from the outset. Patients selected for RT are frequently those clinicians believe are most likely to recur. As a result, observed outcome differences may reflect underlying baseline risk rather than treatment effect. This is the central problem of confounding by indication.
A causal inference framework begins by explicitly modeling this decision process. Rather than treating treatment selection as an inconvenient source of bias, causal inference asks why treatment was selected, which factors influenced that decision, and how those factors also relate to recurrence. Directed acyclic graphs (DAGs) provide one useful approach by requiring investigators to specify the assumed relationships among tumor characteristics, patient characteristics, treatment selection, recurrence outcomes, salvage therapy, and survival before data analysis begins34–36.
In the hypothetical DAG shown in Figure 20, several tumor- and patient-level variables influence both the likelihood of receiving RT and the risk of recurrence. Tumor size, lymphovascular invasion, margin status, primary site, SLNB status, immunosuppression, frailty, and surgical technique may all function as confounders if they affect both treatment selection and recurrence risk. Provider or institutional practice patterns may also influence treatment assignment, radiation fields, fractionation, surgical technique, and surveillance intensity. The red arrow represents the causal effect of interest: the effect of adjuvant RT on recurrence.
NoteFigure 20. Hypothetical causal structure for adjuvant RT in MCC
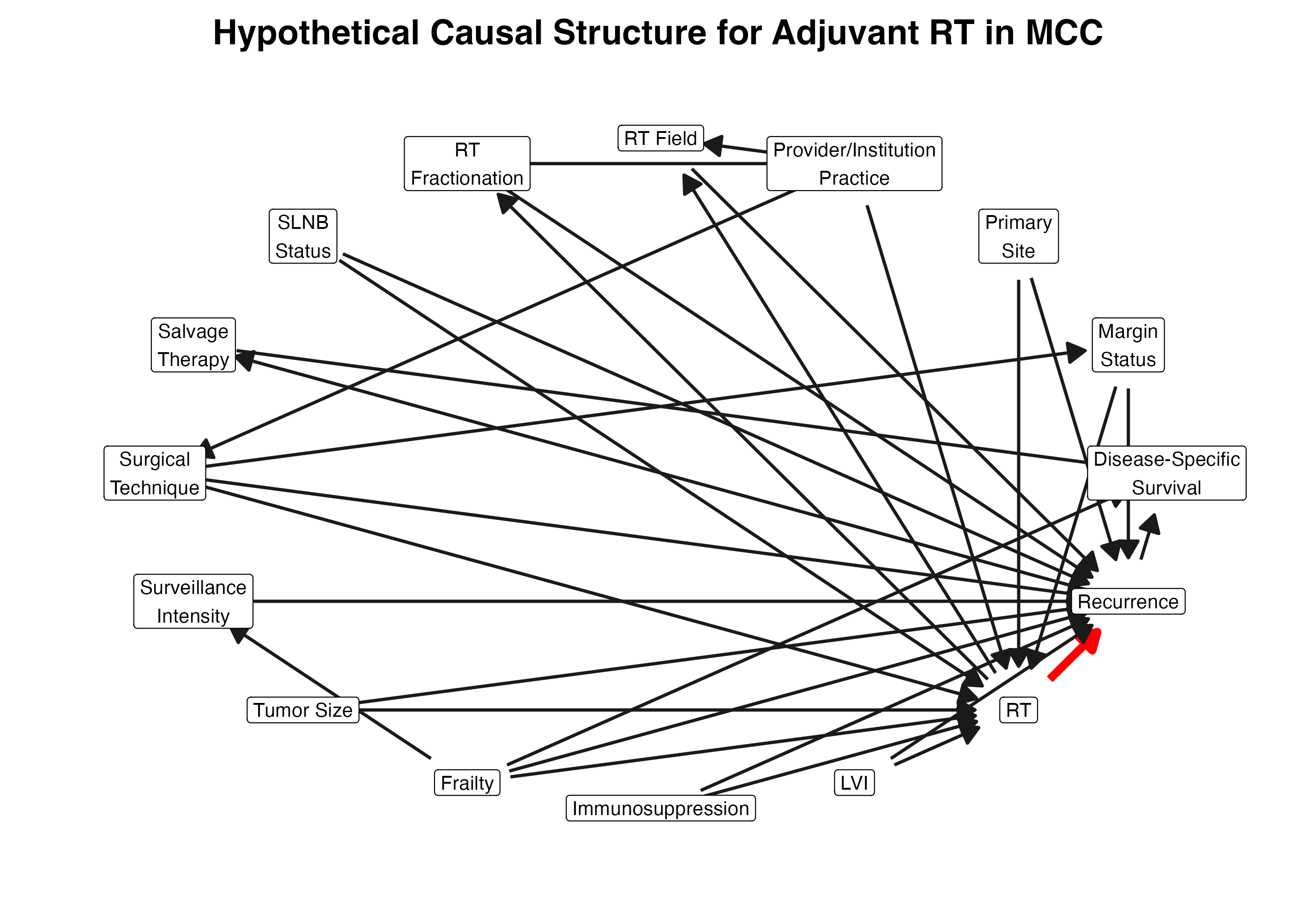
DAGs are useful because they clarify the estimand and help identify adjustment sets: the variables that should be conditioned on to estimate a causal effect under the assumptions encoded in the graph37,38. For example, if tumor size, lymphovascular invasion, primary site, margin status, and immunosuppression influence both RT selection and recurrence, then a naïve comparison of recurrence rates between patients who did and did not receive RT will be biased. Adjustment for these common causes is necessary to estimate the total effect of RT on recurrence. By contrast, variables that occur downstream of RT, such as salvage therapy or post-recurrence survival, should not be adjusted for when estimating the total effect of RT on recurrence, because doing so may block part of the causal pathway or introduce bias.
This distinction is particularly important for multi-institutional MCC evidence generation. A DAG does not prove that the assumed causal structure is correct. Rather, it makes assumptions explicit, transparent, and open to critique. By specifying the causal model before data analysis begins, investigators can determine which variables must be collected, which variables belong in the primary adjustment set, and which variables should be treated as mediators, colliders, post-treatment variables, or downstream outcomes rather than confounders.
Importantly, this approach shifts the focus from asking whether RT and recurrence are associated to estimating the causal effect of RT after accounting for the factors that influenced treatment selection in the first place. For a disease in which treatment decisions are highly individualized, this distinction is critical. Causal inference does not eliminate uncertainty, but it provides a disciplined framework for making that uncertainty explicit and for asking whether the available data can support the clinical question being posed.
Why Probabilistic Models May Be Useful in a Rare Disease
Even with prospective data collection, MCC presents a fundamental inferential challenge: local recurrence is uncommon. Sparse events limit precision, and multicenter studies introduce additional heterogeneity because referral patterns, surgical practice, RT thresholds, fractionation schedules, surveillance intensity, and salvage approaches differ across institutions. Consequently, even thoughtfully designed studies may not produce definitive answers to every clinically important question.
The challenge is therefore not simply to estimate whether RT works on average. Rather, it is to estimate how likely RT is to provide a clinically meaningful benefit for an individual patient. Probabilistic modelsb align naturally with this decision problem because they estimate probabilities that map directly onto clinical decisions. Rather than asking only whether a treatment effect crosses an arbitrary threshold for statistical significance, they estimate the probability that benefit exceeds thresholds clinicians and patients consider meaningful.
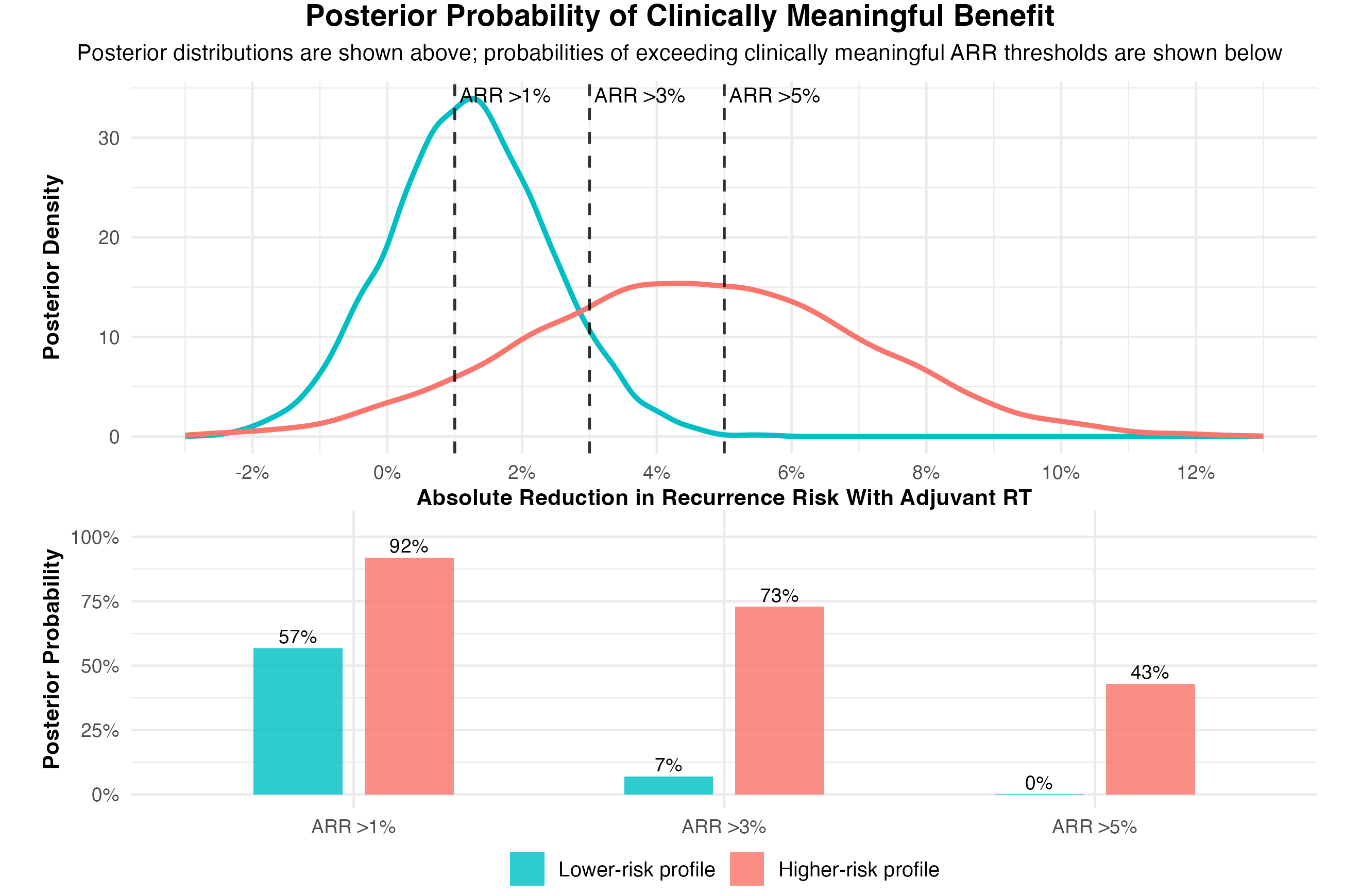
In practical terms, this shifts the question from “Was RT statistically significant?” to “How likely is RT to help enough to justify treatment?” A model could estimate, for example, the probability that RT reduces recurrence risk by more than 1%, 3%, or 5%. Those probabilities can then be considered alongside treatment burden, toxicity, salvageability, patient preferences, and competing risks to support individualized treatment decisions.
Noteb Why Bayesian Analysis May Help Here
In a rare disease, a study may not produce enough events to answer every question with a definitive yes or no.
A Bayesian analysis can still be useful because it estimates probabilities that map directly onto clinical decisions. Instead of asking only whether RT is “statistically significant,” it asks: What is the probability that RT lowers recurrence risk by enough to matter?
This does not eliminate uncertainty. It quantifies uncertainty in a way that is transparent, clinically interpretable, and directly relevant to patient care.
A multicenter MCC study naturally includes several levels of variation: patients differ from one another, and institutions differ in case mix, referral patterns, and treatment practice. A hierarchical Bayesian model provides a way to represent this structure in the analysis. Rather than assuming that all institutions are identical, the model can allow baseline recurrence risk, treatment patterns, and, where data permit, treatment-associated effects to vary across centers.
This approach is particularly useful in rare diseases, where many centers or clinically important subgroups may contribute relatively few patients or events. Through partial pooling, estimates from smaller or sparser groups are informed by the broader multicenter experience, while still allowing larger centers or more data-rich groups to contribute their own information. This helps avoid overfitting to sparse subsets and can produce estimates that are more stable than analyzing each center separately, while avoiding the oversimplification of collapsing all patients into a single undifferentiated dataset.
Hierarchical Bayesian models can also incorporate prior information, including from existing observational studies, and update estimates as new data accrue. This feature is particularly attractive in MCC, where decades of institutional experience already exist but uncertainty remains substantial. At the same time, prior information must be incorporated transparently. Posterior estimates may be sensitive to prior assumptions, particularly when historical evidence arises from studies affected by treatment-selection bias. Accordingly, Bayesian analyses should prespecify prior distributions, justify their selection, and evaluate sensitivity to alternative assumptions.
Importantly, Bayesian modeling does not eliminate confounding, selection bias, or sparse data. Rather, its value is that it expresses the remaining uncertainty in a form that directly informs clinical decision-making. Instead of asking whether uncertainty has been eliminated, clinicians can ask whether the probability of clinically meaningful benefit is sufficient to justify treatment for a particular patient. In this way, probabilistic models help translate imperfect evidence into transparent, individualized decisions.
Visualizing Probabilistic Benefit
This framework addresses a practical question that arose repeatedly throughout our review and discussion: how can rigorous clinical inference continue when important outcomes are uncommon and definitive studies may remain difficult to conduct? One answer is to report decision-relevant probabilities rather than relying solely on a single treatment-effect estimate or a statistical-significance threshold.
The example in Figure 21 is hypothetical rather than derived from observed data. It demonstrates how a prospective hierarchical Bayesian model could estimate the posterior distribution of absolute recurrence reduction with adjuvant RT and summarize the probability that benefit exceeds clinically meaningful thresholds such as 1%, 3%, or 5%. These probabilities can then be interpreted alongside treatment burden, toxicity, salvageability, patient preferences, and other patient-specific considerations. The goal is not to eliminate uncertainty, but to quantify it honestly so that clinicians and patients can make better-informed decisions.
NoteFigure 21. Posterior probability of clinically meaningful benefit
Bayesian Assurance and Study Feasibility
The same probabilistic framework can also be applied before a study begins to evaluate whether a proposed design is likely to produce clinically meaningful evidence. For the illustrative simulations in Table 2, we asked how large a prospective cohort would need to be for a Bayesian analysis to have at least 80% assurance of reaching an actionable conclusion, defined as a greater than 80% posterior probability that the absolute recurrence reduction (ARR) exceeded 3%.
This framing differs from conventional power calculations. Statistical power asks how often a study will detect an effect of a specified size under repeated sampling. Bayesian assurance instead asks how often a proposed study is expected to produce a clinically actionable posterior conclusion, explicitly incorporating uncertainty in the true treatment effect before the study begins. As a result, assurance shifts the emphasis from achieving statistical significance to generating evidence that is sufficiently informative to support clinical decision-making.
NoteTable 2. Arm-specific Bayesian assurance calculations
| Table 2. Bayesian Assurance for Clinically Specified Local-Recurrence Scenarios | ||||||
| Approximate total cohort size needed for each separate comparison design to achieve 80% Bayesian assurance that ARR exceeds 3%. | ||||||
| No RT 1-year LR |
RT 1-year LR |
ARR | Relative risk reduction |
Approximate total prospective cohort size, patients (separate comparison designs; do not sum across columns) |
||
|---|---|---|---|---|---|---|
| Any RT (65%) vs no RT (35%) |
Conventional or hypofractionated RT (each 25%) vs no RT (35%) |
Single-fraction RT (15%) vs no RT (35%) |
||||
| 5% | 1% | 4% | 80% | 5,000 | 8,000 | 6,000 |
| 10% | 5% | 5% | 50% | 3,000 | 3,000 | 5,000 |
| 10% | 2% | 8% | 80% | 400 | 400 | 600 |
| 10% | 1% | 9% | 90% | 200 | 300 | 400 |
| 20% | 10% | 10% | 50% | 400 | 500 | 800 |
| 20% | 5% | 15% | 75% | 200 | 200 | 200 |
| Values in the three rightmost columns are alternative design scenarios for separate pairwise comparisons and should not be summed across columns. Each value represents the approximate total prospective cohort size in patients needed to achieve 80% Bayesian assurance for that comparison design. Candidate total cohort sizes were evaluated from 100 to 10,000 patients. | ||||||
| Allocation assumptions are shown in the column headers and are expressed as percentages of the full prospective capture cohort. The conventional/hypofractionated column models conventional RT and hypofractionated RT as separate arms with identical 25% allocation and operating characteristics; it is not a pooled 50% multi-fraction comparison. For arm-specific comparisons, patients receiving other RT regimens are captured in the total cohort but do not contribute to that pairwise contrast; therefore, the reported values should be read as total cohort sizes, not per-arm sample sizes. | ||||||
| Scenarios with ARR ≤3% are not shown because a rule requiring Pr(ARR >3%) >80% is not expected to achieve 80% assurance when the true effect is at or below 3%. High-benefit scenarios, including 20% → 5%, are illustrative data-generating assumptions rather than predictions. | ||||||
Table 2. Scenario-based Bayesian assurance calculations using local recurrence as the endpoint. Values represent the approximate total prospective cohort size required to achieve at least 80% Bayesian assurance under each clinically specified local-recurrence scenario. Bayesian assurance was defined as the proportion of simulated future studies that met a prespecified posterior decision rule. For these simulations, the clinically meaningful effect threshold was an absolute risk reduction (ARR) greater than 3%, and the posterior decision rule required greater than 80% posterior probability that ARR exceeded this threshold.
For each scenario, we specified assumed 1-year local recurrence risks with and without primary-site RT, which together define the corresponding ARR and relative risk reduction. Simulated studies were then generated across a prespecified grid of total cohort sizes ranging from 100 to 10,000 patients. Within each simulated study, patients were allocated according to prespecified comparison-specific proportions: 35% no RT, 65% any RT pooled, 25% conventional RT or hypofractionated RT, each modeled separately with identical allocation and operating characteristics, and 15% single-fraction RT. These allocation assumptions are part of the design being evaluated; different treatment distributions would produce different assurance estimates and sample-size requirements.
For each simulated study, beta-binomial posterior updating was used to estimate the probability that ARR exceeded the clinically meaningful threshold of 3%. A simulated study was considered clinically actionable if this posterior probability exceeded 80%. The table reports the smallest total cohort size at which at least 80% of simulated studies satisfied this decision rule.
These values should be interpreted as approximate operating characteristics of a proposed study design rather than exact sample-size requirements. Assurance summarizes how often a proposed design is expected to yield a clinically actionable posterior conclusion across many possible future studies, not whether any single realized study will necessarily do so. Individual studies conducted under the same design may still produce stronger or weaker posterior evidence because of sparse events, random variation, or differences in the observed distribution of patients across treatment groups.
Scenarios in which the true ARR is at or below the clinically meaningful threshold of 3% are not shown because increasing sample size would be expected to concentrate the posterior at or below that threshold, rather than increase the probability that ARR exceeds it. This observation illustrates an important principle of study design. When the untreated baseline risk of local recurrence is very low—as suggested by the Kavanagh cohort—a large absolute benefit from RT may simply not be biologically possible. In that setting, the scientific objective shifts. Rather than attempting to demonstrate a clinically meaningful absolute benefit, the more informative question becomes whether the available evidence can confidently exclude such a benefit for selected patients.
Framed this way, Bayesian assurance helps determine not only when a study is likely to demonstrate a clinically meaningful reduction in local recurrence, but also when it is likely to provide sufficiently informative evidence to support treatment de-escalation. However, because these calculations use local recurrence as the endpoint, they do not by themselves establish whether primary-site RT improves disease-specific survival or overall survival. This distinction is clinically important: if local recurrences are uncommon and effectively salvageable, then a reduction in recurrence may not translate into improved disease-specific outcomes. In that setting, the clinical value of routine adjuvant treatment should be judged not only by the magnitude of recurrence reduction, but also by salvageability, toxicity, treatment burden, competing risks, and patient preferences.
Although the scenario-based assurance calculations focus on local recurrence, the broader framework extends to any clinically relevant outcome. A curated multi-institutional evidence-generation effort should evaluate not only local recurrence, but also regional and locoregional recurrence, recurrence-free or progression-free survival, overall survival, salvageability, toxicity, treatment burden, and patient preferences. Local recurrence serves as a useful modeled endpoint because it is directly relevant to the Kavanagh study and to the intended effect of primary-site RT. More broadly, however, study feasibility for any endpoint depends on the underlying event rate, the expected absolute treatment effect, treatment allocation, and the degree of uncertainty investigators and clinicians are willing to accept.
This perspective differs from conventional sample-size or power calculations. Traditional power calculations ask how many patients are required to reject a null hypothesis under prespecified assumptions about the true treatment effect and type I error. Bayesian assurance instead asks how often a proposed study design is expected to produce evidence that is sufficiently informative to support a prespecified clinical decision. In this framework, the objective shifts from achieving statistical significance to generating clinically actionable evidence.
This distinction is particularly relevant in rare diseases. If the true absolute benefit of RT is large—for example, a reduction in 1-year local recurrence from 10% to 1%—a prospective study may produce informative evidence with only a few hundred patients. If the true ARR is closer to 5%, several thousand patients may be required, particularly for less commonly used treatment approaches such as single-fraction RT. Conversely, if the true ARR is closer to 1%, even a large study may be unlikely to demonstrate that benefit exceeds commonly accepted clinical thresholds, despite supporting the existence of a small treatment effect.
This illustrates why accurately characterizing the natural history of local recurrence is so important. The maximum achievable absolute benefit of RT is constrained by the baseline recurrence risk. If the untreated 1-year local recurrence risk is approximately 2%, as reported by Kavanagh et al., then an ARR greater than 3% is mathematically impossible for local recurrence, even if RT completely eliminated all local failures. In that setting, the scientific objective shifts from demonstrating a large absolute benefit to more precisely estimating baseline risk, identifying patients most likely to benefit, and determining how confidently clinically meaningful benefit can be excluded for selected low-risk patients. Even when a prespecified benefit threshold is unlikely to be exceeded, posterior probabilities remain informative by clarifying what is likely, unlikely, and still uncertain.
From Recurrence Rates to Decision Quality
Ultimately, the goal of future evidence generation is not simply to estimate local recurrence more precisely, but to improve clinical decision-making. Patients and clinicians need to know which individuals can safely omit RT, which patients are likely to benefit from treatment, whether abbreviated RT provides an acceptable balance of benefit and burden, and how recurrence risk should be weighed alongside salvageability, toxicity, competing risks, and patient preferences.
No single study is likely to eliminate uncertainty, particularly in a rare disease characterized by low event rates, evolving treatment practices, and heterogeneous clinical decision-making. That should not be interpreted as failure. The value of a study lies not only in producing definitive answers, but also in reducing uncertainty, refining clinically important estimates, and improving the decisions that clinicians and patients make together. By making assumptions explicit and quantifying uncertainty transparently, causal inference and probabilistic modeling provide a framework for learning even when definitive answers remain out of reach.
Conclusion
The study by Kavanagh et al. has prompted an important reexamination of adjuvant primary-site RT following complete excision of localized MCC. The low local recurrence rates reported in their cohort challenge prevailing assumptions, but the broader controversy extends beyond any single recurrence estimate. It reflects unresolved questions regarding baseline risk, treatment selection, clinically meaningful benefit, recurrence salvageability, treatment burden, and patient preferences.
The SoCO Journal Club demonstrated that these uncertainties are reflected in contemporary practice. Although clinicians broadly agree on many of the factors that influence risk, substantial variation remains in how recurrence risk is estimated, how treatment benefit is judged, and what level of uncertainty is acceptable when recommending RT.
Future evidence generation should therefore focus not simply on collecting more data, but on generating more informative evidence. Curated multi-institutional data collection, standardized recurrence definitions, explicit causal frameworks, and probabilistic models offer complementary approaches for estimating individualized treatment benefit while acknowledging the realities of studying a rare disease.
Perhaps the most important contribution of the Kavanagh study is not that it resolves the controversy surrounding adjuvant RT, but that it clarifies the uncertainty that remains. For rare diseases such as MCC, the perfect study may never arrive. Scientific rigor, then, is not the pursuit of certainty; it is the disciplined quantification of uncertainty. Progress comes from measuring uncertainty honestly, communicating it transparently, and incorporating it into better clinical decisions.
Materials and Methods
Bibliography
Appendix
NoteAbbreviations, Acknowledgments, Citation, Disclaimer, Disclosures, License, Publication Stage
Abbreviations
AJCC, American Joint Committee on Cancer; ADMEC-O, Adjuvant Avelumab in Merkel Cell Carcinoma trial; APP, advanced practice provider; ARR, absolute risk reduction; CI, confidence interval; DAG, directed acyclic graph; DeCOG, Dermatologic Cooperative Oncology Group; DFS, disease-free survival; DSS, disease-specific survival; ENT, ear, nose, and throat; HR, hazard ratio; LN, lymph node; LR, local recurrence; LVI, lymphovascular invasion; MCC, Merkel cell carcinoma; MSKCC, Memorial Sloan Kettering Cancer Center; NCDB, National Cancer Database; NCCN, National Comprehensive Cancer Network; OR, odds ratio; OS, overall survival; Pr, probability; RFS, recurrence-free survival; RT, radiation therapy; SEER, Surveillance, Epidemiology, and End Results; SLN, sentinel lymph node; SLNB, sentinel lymph node biopsy; SoCO, Society of Cutaneous Oncology; VA, Veterans Affairs; WLE, wide local excision.
Acknowledgments
The authors thank the members of the Society of Cutaneous Oncology community who participated in the June 12, 2026 Journal Club. Their thoughtful discussion, clinical perspectives, and survey responses directly informed the questions, analyses, and recommendations developed in this Perspectives article.
Citation
For attribution, please cite this work as:
Miller DM, Emerick KS, Kaufman HL, McEvoy AM, Zaba L, Sharma A, Adelaja A, Silk AW, Khushalani NI, Brownell I, Coit DG, Nghiem P, Sondak VK. Local Recurrence After Excision of Merkel Cell Carcinoma: What Do We Actually Know, and What Should We Do Next? Journal of Cutaneous Oncology. 2026;4(2). https://doi.org/10.59449/joco.2026.07.16 Copied!
BibTeX citation:
@article{miller2026localrecurrence,
author = {Miller, David Michael and Emerick, Kevin Scott and Kaufman, Howard Lane and McEvoy, Aubriana M. and Zaba, Lisa and Sharma, Ajay and Adelaja, Ade and Silk, Ann W. and Khushalani, Nikhil I. and Brownell, Isaac and Coit, Daniel G. and Nghiem, Paul and Sondak, Vernon K.},
title = {Local Recurrence After Excision of Merkel Cell Carcinoma: What Do We Actually Know, and What Should We Do Next?},
journal = {Journal of Cutaneous Oncology},
year = {2026},
volume = {4},
number = {2},
url = {https://journalofcutaneousoncology.io/perspectives/Vol_4_Issue_2/Local_Recurrence_After_Excision_MCC/},
doi = {10.59449/joco.2026.07.16},
issn = {2837-1933},
publisher = {Society of Cutaneous Oncology},
langid = {en}
}Disclaimer
This site represents our opinions only. See our full Disclaimer
Disclosures
Conflict of Interests
Dr. Miller has received honoraria for serving as a consultant or participating on advisory boards for Almirall, Bristol Myers Squibb, Merck, EMD Serono, Regeneron, Sanofi Genzyme, Pfizer, Castle Biosciences, Checkpoint Therapeutics, and Sun Pharma. He serves on the Unloxcyt steering committee for Sun Pharma. He has stock options from Avstera Therapeutics. He has received institutional research funding from Regeneron, Kartos Therapeutics, NeoImmune Tech, Inc., Project Data Sphere, ECOG-ACRIN, and the American Skin Association.
Dr. Khushalani owns stock in Asensus Surgical, and Bellicum Pharmaceuticals. He participates in data and safety monitoring for AstraZeneca and Incyte Corporation. He has served as a consultant for Bristol Myers Squibb, Castle Biosciences, IDEAYA Biosciences, Immunocore, Instil Bio, IO Biotech, Iovance Biotherapeutics, Merck, Mural Oncology, MyCareGorithm, Nektar, Novartis, Regeneron Pharmaceuticals, Replimune, T-Knife Therapeutics, Delcath, and Sun Pharmaceuticals.
Dr. Nghiem reports compensation/support from UpToDate (honoraria), Almirall (advisory role), Incyte (institutional research funding), and has a patent pending for high-affinity T-cell receptors that target the Merkel polyomavirus, Patent filed: “Merkel cell polyomavirus T antigen-specific TCRs and uses thereof” (institution).
Dr. Kaufman is an employee of Ankyra Therapeutics. He has served in advisory roles for Castle Biosciences, Marengo Therapeutics, Tatum Biosciences, and Virogin Biotech; serves on the Board of Crichton Biosciences; holds stock in Replimune, Inc.; and has received honoraria from the Society for Immunotherapy of Cancer.
Dr. Sondak is a compensated consultant for Bristol Myers Squibb, Merck, and Mural Oncology, and receives research funding from Neogene Therapeutics and Skyline.
Dr. Emerick reports advisory board honoraria from Regeneron, royalties from UpToDate, and research funding from Haystack.
Dr. Silk reports receiving grants/research support to her institution from Regeneron and Merck, advisory board fees from Merck and Regeneron, and royalties from UpToDate, Inc.
Drs. Coit, McEvoy, Zaba, Sharma, Adelaja, and Brownell report no relevant disclosures.
License
This work is licensed under a creative commons BY-NC-ND license

Publication Stage
- Published